

Mechanical Complications of Acute Myocardial Infarction: A Scientific Statement From the American Heart Association
- PMID: 34126755
- PMCID: PMC9364424
- DOI: 10.1161/CIR.0000000000000985
Mechanical Complications of Acute Myocardial Infarction: A Scientific Statement From the American Heart Association
Abstract
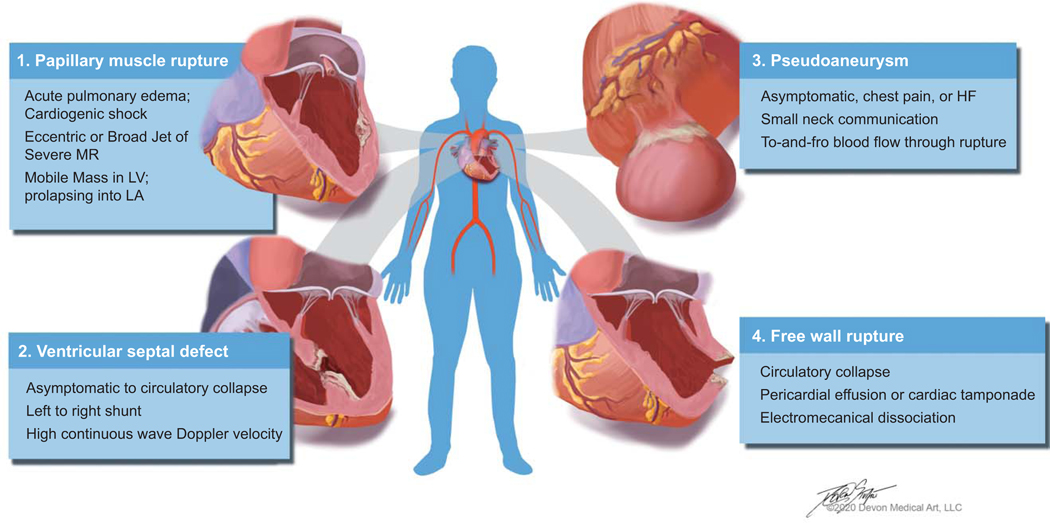
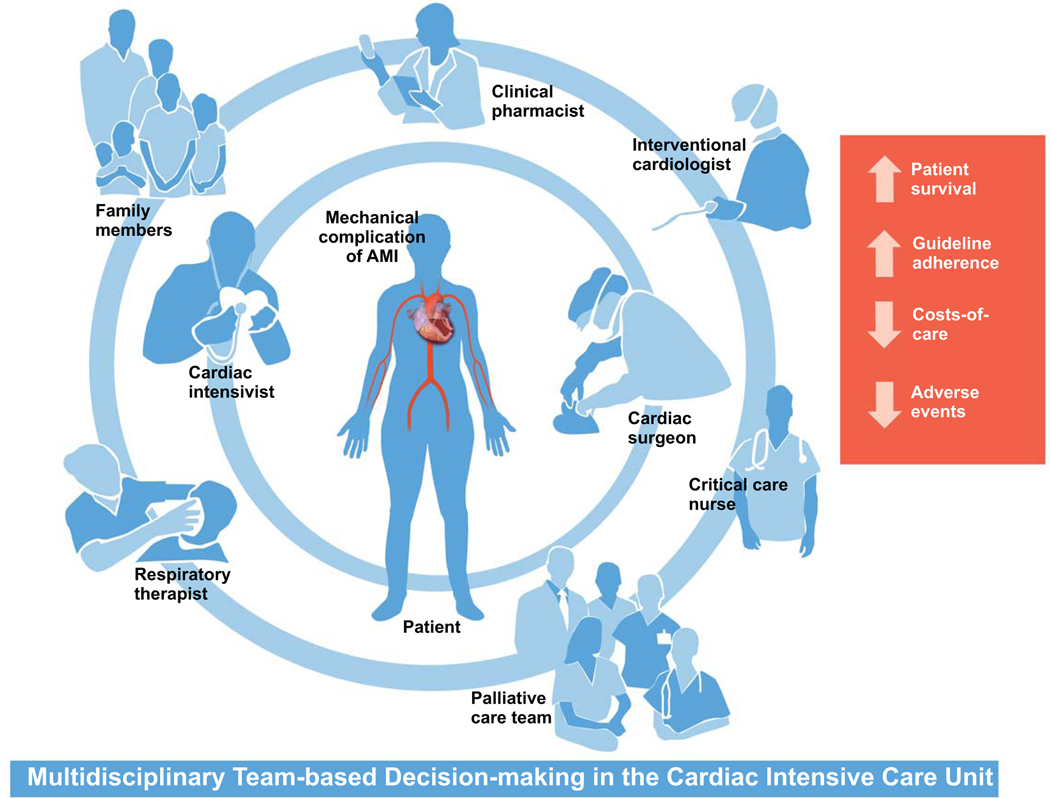
Over the past few decades, advances in pharmacological, catheter-based, and surgical reperfusion have improved outcomes for patients with acute myocardial infarctions. However, patients with large infarcts or those who do not receive timely revascularization remain at risk for mechanical complications of acute myocardial infarction. The most commonly encountered mechanical complications are acute mitral regurgitation secondary to papillary muscle rupture, ventricular septal defect, pseudoaneurysm, and free wall rupture; each complication is associated with a significant risk of morbidity, mortality, and hospital resource utilization. The care for patients with mechanical complications is complex and requires a multidisciplinary collaboration for prompt recognition, diagnosis, hemodynamic stabilization, and decision support to assist patients and families in the selection of definitive therapies or palliation. However, because of the relatively small number of high-quality studies that exist to guide clinical practice, there is significant variability in care that mainly depends on local expertise and available resources.
Keywords: AHA Scientific Statements; ST-segment–elevation myocardial infarction; aging; heart rupture; heart septal defects; mitral valve insufficiency; percutaneous coronary intervention; reperfusion; ventricular.
Figures


References
-
- Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, Chiuve SE, Cushman M, Delling FN, Deo R, de Ferranti SD, Ferguson JF, Fornage M, Gillespie C, Isasi CR, Jimenez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Lutsey PL, Mackey JS, Matchar DB, Matsushita K, Mussolino ME, Nasir K, O’Flaherty M, Palaniappan LP, Pandey A, Pandey DK, Reeves MJ, Ritchey MD, Rodriguez CJ, Roth GA, Rosamond WD, Sampson UKA, Satou GM, Shah SH, Spartano NL, Tirschwell DL, Tsao CW, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS, Muntner P, American Heart Association Council on E, Prevention Statistics C and Stroke Statistics S. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation. 2018;137:e67–e492. - PubMed
-
- Damluji AA, Bandeen-Roche K, Berkower C, Boyd CM, Al-Damluji MS, Cohen MG, Forman DE, Chaudhary R, Gerstenblith G, Walston JD, Resar JR and Moscucci M. Percutaneous Coronary Intervention in Older Patients With ST-Segment Elevation Myocardial Infarction and Cardiogenic Shock. J Am Coll Cardiol. 2019;73:1890–1900. - PMC - PubMed
-
- Peterson ED, Shah BR, Parsons L, Pollack CV Jr., French WJ, Canto JG, Gibson CM and Rogers WJ. Trends in quality of care for patients with acute myocardial infarction in the National Registry of Myocardial Infarction from 1990 to 2006. Am Heart J. 2008;156:1045–55. - PubMed
-
- Damluji AA, Forman DE, van Diepen S, Alexander KP, Page RL 2nd, Hummel SL, Menon V, Katz JN, Albert NM, Afilalo J, Cohen MG, American Heart Association Council on Clinical C, Council on C and Stroke N. Older Adults in the Cardiac Intensive Care Unit: Factoring Geriatric Syndromes in the Management, Prognosis, and Process of Care: A Scientific Statement From the American Heart Association. Circulation. 2020;141:e6–e32. - PubMed
-
- O’Gara PT, Kushner FG, Ascheim DD, Casey DE Jr, Chung MK, de Lemos JA, Ettinger SM, Fang JC, Fesmire FM, Franklin BA, Granger CB, Krumholz HM, Linderbaum JA, Morrow DA, Newby LK, Ornato JP, Ou N, Radford MJ, Tamis-Holland JE, Tommaso CL, Tracy CM, Woo YJ, Zhao DX, Anderson JL, Jacobs AK, Halperin JL, Albert NM, Brindis RG, Creager MA, DeMets D, Guyton RA, Hochman JS, Kovacs RJ, Kushner FG, Ohman EM, Stevenson WG, Yancy CW and American College of Cardiology Foundation/American Heart Association Task Force on Practice G. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:e362–425. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
