

Deep Learning to Predict Cardiac Magnetic Resonance-Derived Left Ventricular Mass and Hypertrophy From 12-Lead ECGs
- PMID: 34126762
- PMCID: PMC8217289
- DOI: 10.1161/CIRCIMAGING.120.012281
Deep Learning to Predict Cardiac Magnetic Resonance-Derived Left Ventricular Mass and Hypertrophy From 12-Lead ECGs
Abstract
Background: Classical methods for detecting left ventricular (LV) hypertrophy (LVH) using 12-lead ECGs are insensitive. Deep learning models using ECG to infer cardiac magnetic resonance (CMR)-derived LV mass may improve LVH detection.
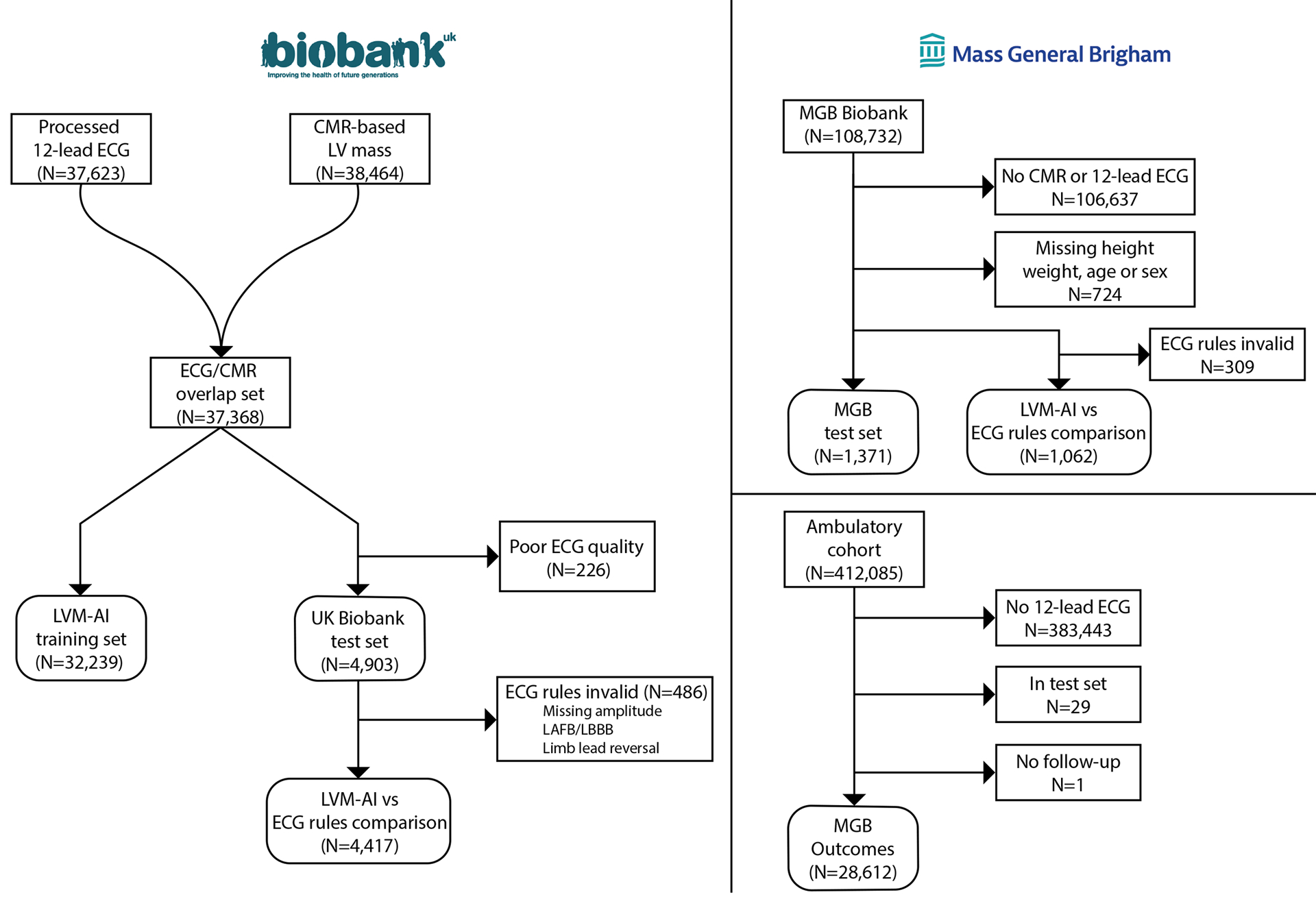
Methods: Within 32 239 individuals of the UK Biobank prospective cohort who underwent CMR and 12-lead ECG, we trained a convolutional neural network to predict CMR-derived LV mass using 12-lead ECGs (left ventricular mass-artificial intelligence [LVM-AI]). In independent test sets (UK Biobank [n=4903] and Mass General Brigham [MGB, n=1371]), we assessed correlation between LVM-AI predicted and CMR-derived LV mass and compared LVH discrimination using LVM-AI versus traditional ECG-based rules (ie, Sokolow-Lyon, Cornell, lead aVL rule, or any ECG rule). In the UK Biobank and an ambulatory MGB cohort (MGB outcomes, n=28 612), we assessed associations between LVM-AI predicted LVH and incident cardiovascular outcomes using age- and sex-adjusted Cox regression.
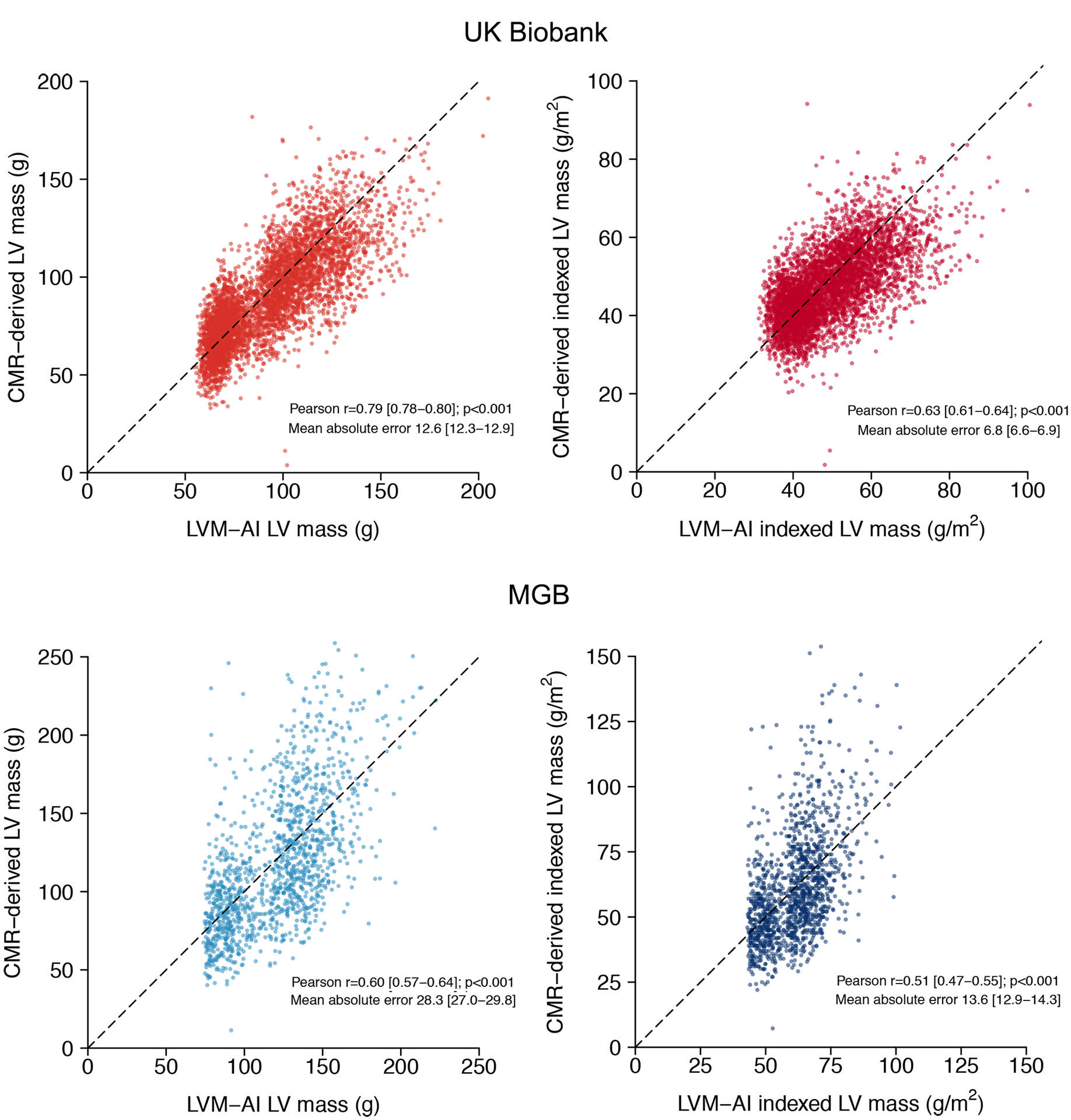
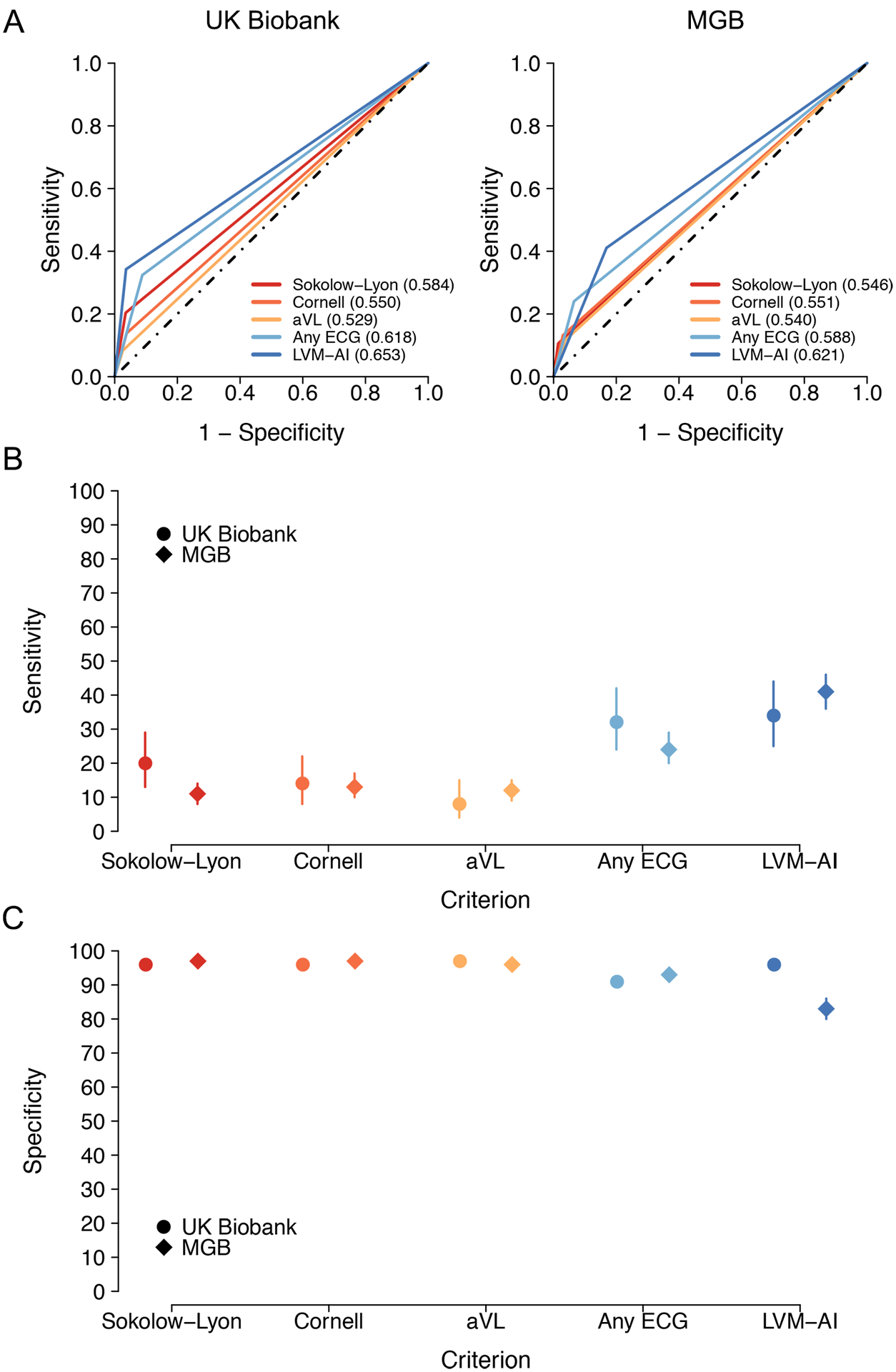
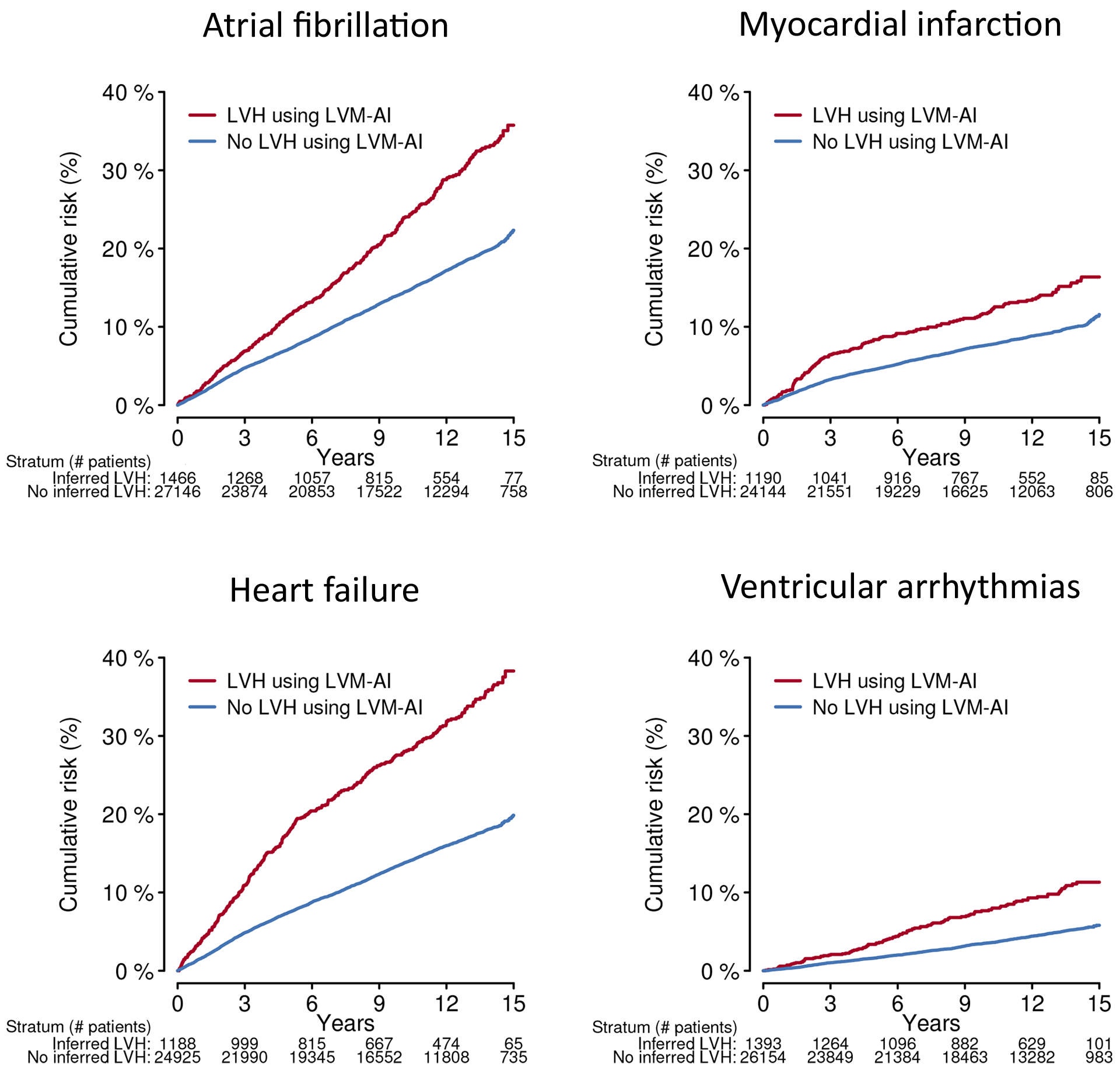
Results: LVM-AI predicted LV mass correlated with CMR-derived LV mass in both test sets, although correlation was greater in the UK Biobank (r=0.79) versus MGB (r=0.60, P<0.001 for both). When compared with any ECG rule, LVM-AI demonstrated similar LVH discrimination in the UK Biobank (LVM-AI c-statistic 0.653 [95% CI, 0.608 -0.698] versus any ECG rule c-statistic 0.618 [95% CI, 0.574 -0.663], P=0.11) and superior discrimination in MGB (0.621; 95% CI, 0.592 -0.649 versus 0.588; 95% CI, 0.564 -0.611, P=0.02). LVM-AI-predicted LVH was associated with incident atrial fibrillation, myocardial infarction, heart failure, and ventricular arrhythmias.
Conclusions: Deep learning-inferred LV mass estimates from 12-lead ECGs correlate with CMR-derived LV mass, associate with incident cardiovascular disease, and may improve LVH discrimination compared to traditional ECG rules.
Keywords: atrial fibrillation; heart failure; left ventricular hypertrophy; machine learning; myocardial infarction.
Figures

Comment in
-
ECG for Screening Cardiac Abnormalities: The Premise and Promise of Machine Learning.Circ Cardiovasc Imaging. 2021 Jun;14(6):e012837. doi: 10.1161/CIRCIMAGING.121.012837. Epub 2021 Jun 15. Circ Cardiovasc Imaging. 2021. PMID: 34129345 No abstract available.
References
-
- Chrispin J, Jain A, Soliman EZ, Guallar E, Alonso A, Heckbert SR, Bluemke DA, Lima JAC, Nazarian S. Association of electrocardiographic and imaging surrogates of left ventricular hypertrophy with incident atrial fibrillation: MESA (Multi-Ethnic Study of Atherosclerosis). J Am Coll Cardiol. 2014;63:2007–2013. - PMC - PubMed
-
- Casale PN, Devereux RB, Kligfield P, Eisenberg RR, Miller DH, Chaudhary BS, Phillips MC. Electrocardiographic detection of left ventricular hypertrophy: development and prospective validation of improved criteria. J Am Coll Cardiol. 1985;6:572–580. - PubMed
-
- Sokolow M, Lyon TP. The ventricular complex in left ventricular hypertrophy as obtained by unipolar precordial and limb leads. Am Heart J. 1949;37:161–186. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
