

Investigating the drivers of the spatio-temporal heterogeneity in COVID-19 hospital incidence-Belgium as a study case
- PMID: 34127000
- PMCID: PMC8200785
- DOI: 10.1186/s12942-021-00281-1
Investigating the drivers of the spatio-temporal heterogeneity in COVID-19 hospital incidence-Belgium as a study case
Abstract
Background: The COVID-19 pandemic is affecting nations globally, but with an impact exhibiting significant spatial and temporal variation at the sub-national level. Identifying and disentangling the drivers of resulting hospitalisation incidence at the local scale is key to predict, mitigate and manage epidemic surges, but also to develop targeted measures. However, this type of analysis is often not possible because of the lack of spatially-explicit health data and spatial uncertainties associated with infection.
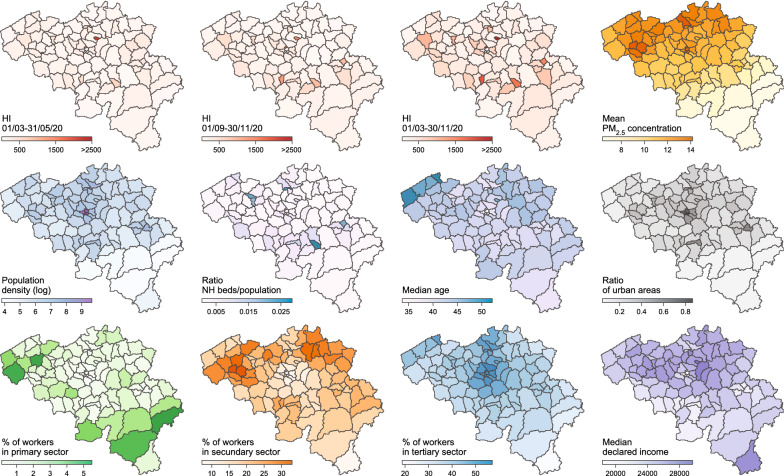
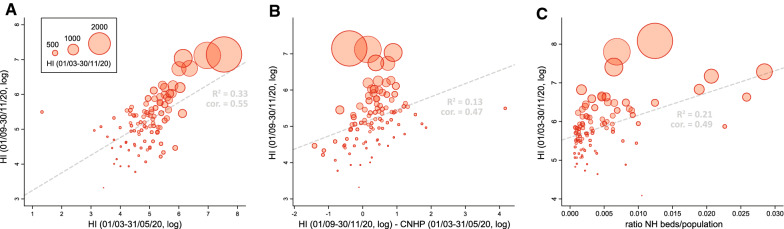
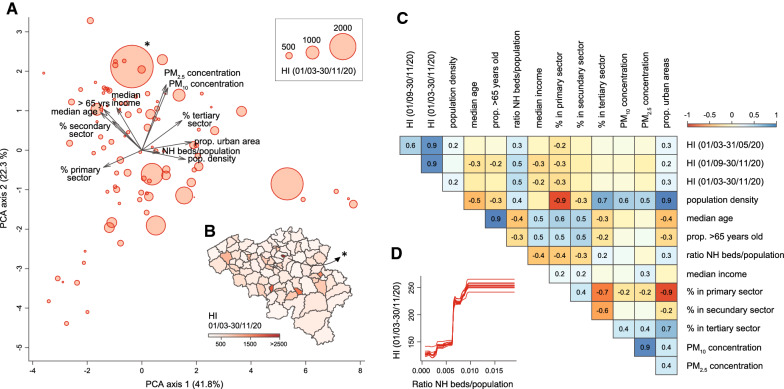
Methods: To overcome these limitations, we propose an analytical framework to investigate potential drivers of the spatio-temporal heterogeneity in COVID-19 hospitalisation incidence when data are only available at the hospital level. Specifically, the approach is based on the delimitation of hospital catchment areas, which allows analysing associations between hospitalisation incidence and spatial or temporal covariates. We illustrate and apply our analytical framework to Belgium, a country heavily impacted by two COVID-19 epidemic waves in 2020, both in terms of mortality and hospitalisation incidence.
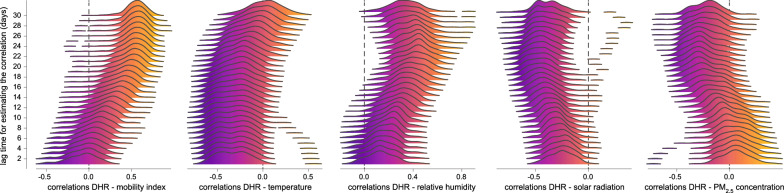
Results: Our spatial analyses reveal an association between the hospitalisation incidence and the local density of nursing home residents, which confirms the important impact of COVID-19 in elderly communities of Belgium. Our temporal analyses further indicate a pronounced seasonality in hospitalisation incidence associated with the seasonality of weather variables. Taking advantage of these associations, we discuss the feasibility of predictive models based on machine learning to predict future hospitalisation incidence.
Conclusion: Our reproducible analytical workflow allows performing spatially-explicit analyses of data aggregated at the hospital level and can be used to explore potential drivers and dynamic of COVID-19 hospitalisation incidence at regional or national scales.
Keywords: Belgium; Boosted regression trees; COVID-19; Hospitalisation incidence; Spatial covariates; Temporal covariates.
Conflict of interest statement
The authors declare no competing interest.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
