

Serum uric acid, disease severity and outcomes in COVID-19
- PMID: 34127048
- PMCID: PMC8201458
- DOI: 10.1186/s13054-021-03616-3
Serum uric acid, disease severity and outcomes in COVID-19
Abstract
Background: The severity of coronavirus disease 2019 (COVID-19) is highly variable between individuals, ranging from asymptomatic infection to critical disease with acute respiratory distress syndrome requiring mechanical ventilation. Such variability stresses the need for novel biomarkers associated with disease outcome. As SARS-CoV-2 infection causes a kidney proximal tubule dysfunction with urinary loss of uric acid, we hypothesized that low serum levels of uric acid (hypouricemia) may be associated with severity and outcome of COVID-19.
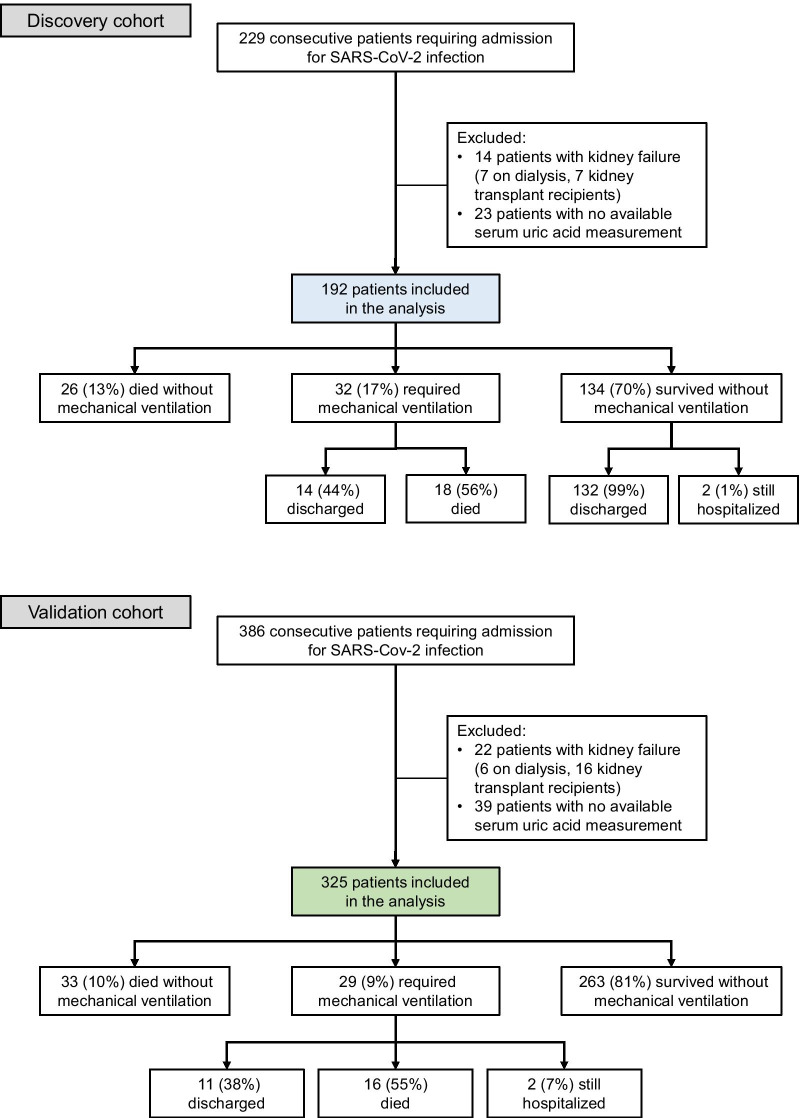
Methods: In a retrospective study using two independent cohorts, we investigated and validated the prevalence, kinetics and clinical correlates of hypouricemia among patients hospitalized with COVID-19 to a large academic hospital in Brussels, Belgium. Survival analyses using Cox regression and a competing risk approach assessed the time to mechanical ventilation and/or death. Confocal microscopy assessed the expression of urate transporter URAT1 in kidney proximal tubule cells from patients who died from COVID-19.
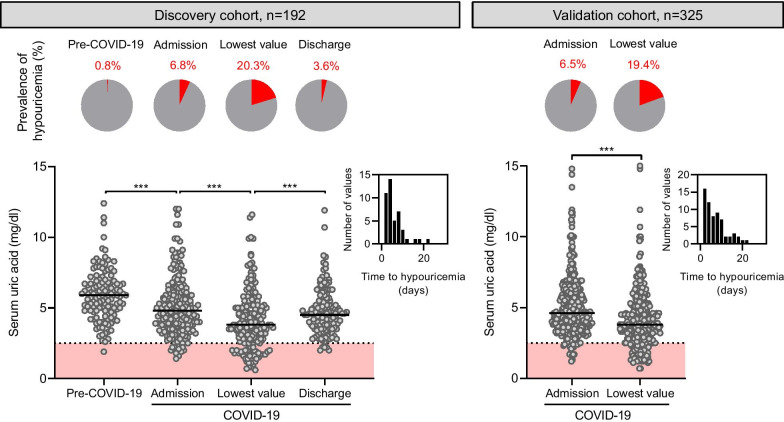
Results: The discovery and validation cohorts included 192 and 325 patients hospitalized with COVID-19, respectively. Out of the 517 patients, 274 (53%) had severe and 92 (18%) critical COVID-19. In both cohorts, the prevalence of hypouricemia increased from 6% upon admission to 20% within the first days of hospitalization for COVID-19, contrasting with a very rare occurrence (< 1%) before hospitalization for COVID-19. During a median (interquartile range) follow-up of 148 days (50-168), 61 (12%) patients required mechanical ventilation and 93 (18%) died. In both cohorts considered separately and in pooled analyses, low serum levels of uric acid were strongly associated with disease severity (linear trend, P < 0.001) and with progression to death and respiratory failure requiring mechanical ventilation in Cox (adjusted hazard ratio 5.3, 95% confidence interval 3.6-7.8, P < 0.001) or competing risks (adjusted hazard ratio 20.8, 95% confidence interval 10.4-41.4, P < 0.001) models. At the structural level, kidneys from patients with COVID-19 showed a major reduction in urate transporter URAT1 expression in the brush border of proximal tubules.
Conclusions: Among patients with COVID-19 requiring hospitalization, low serum levels of uric acid are common and associate with disease severity and with progression to respiratory failure requiring invasive mechanical ventilation.
Keywords: Acute respiratory distress syndrome; Hypouricemia; Mechanical ventilation; Proximal tubule; SARS-CoV-2.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
