

Use and disparities in parathyroidectomy for symptomatic primary hyperparathyroidism in the Medicare population
- PMID: 34127301
- PMCID: PMC8550999
- DOI: 10.1016/j.surg.2021.05.026
Use and disparities in parathyroidectomy for symptomatic primary hyperparathyroidism in the Medicare population
Abstract
Background: Few studies assess use of parathyroidectomy among older adults with symptomatic primary hyperparathyroidism. Our objective was to determine national usage and disparities in parathyroidectomy for symptomatic primary hyperparathyroidism among insured older adults.
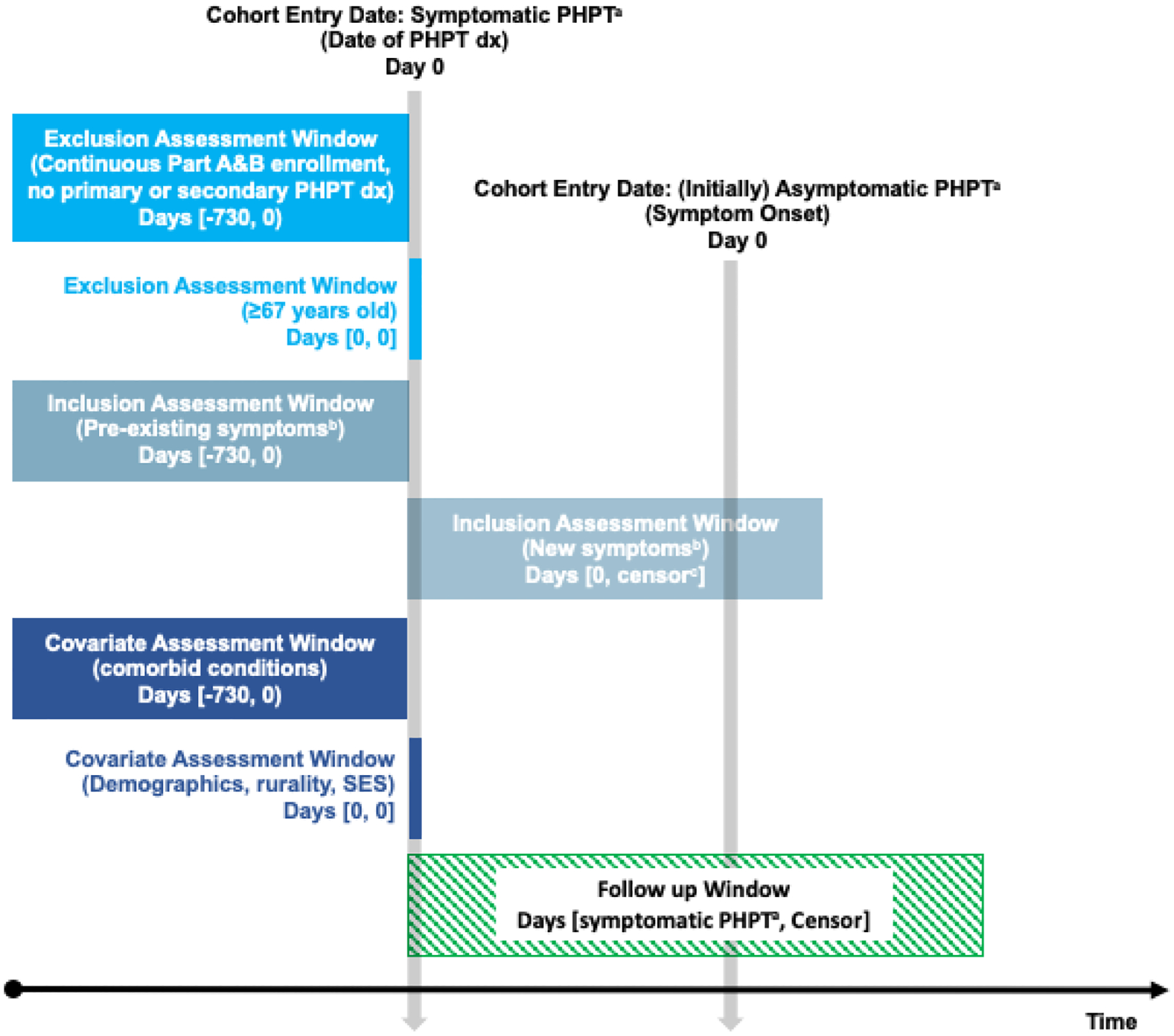
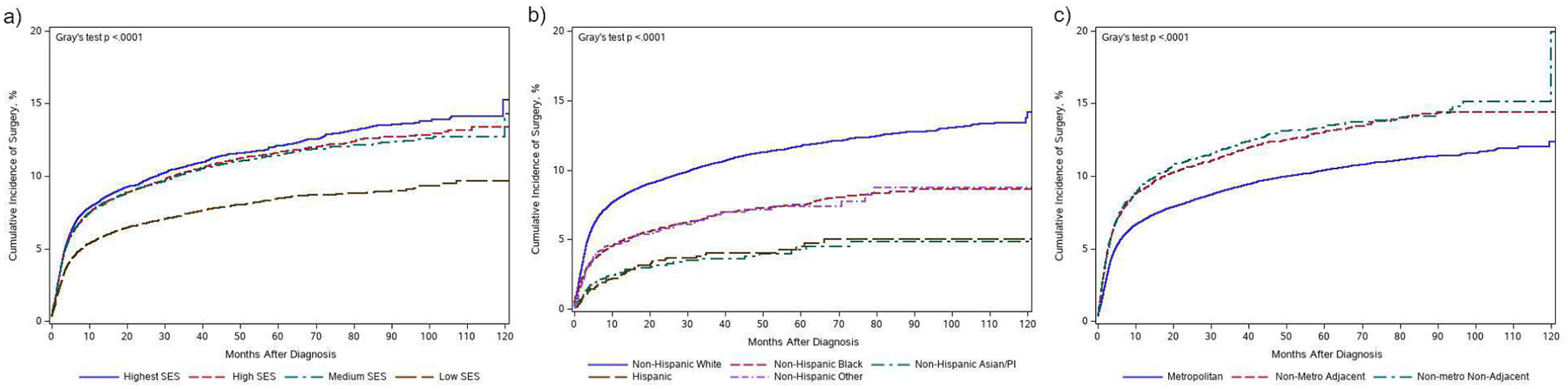
Methods: We identified older adult patients with symptomatic primary hyperparathyroidism using Medicare claims (2006-2017). Primary study variables were race/ethnicity, rurality, and zip-code socioeconomic status. We calculated cumulative incidence of parathyroidectomy and used multivariable Cox proportional hazards regression models to assess the adjusted association of our study variables with parathyroidectomy.
Results: We included 94,803 patients. The median age at primary hyperparathyroidism diagnosis was 76 years (interquartile range 71-82). The majority of patients were female (72%), non-Hispanic White (82%), from metropolitan areas (82%), and had a Charlson Comorbidity score ≥3 (62%). Nine percent of patients (n = 8,251) underwent parathyroidectomy during follow-up. After adjustment, non-Hispanic Black patients, compared to non-Hispanic White (hazard ratio 0.80; 95% confidence interval 0.74, 0.87), and living in a low socioeconomic status neighborhood (low socioeconomic status vs highest socioeconomic status hazard ratio 0.89; 95% confidence interval 0.83, 0.95) were both associated with lower incidences of parathyroidectomy. Patients from non-metropolitan areas were more likely to undergo parathyroidectomy.
Conclusion: Parathyroidectomy is underused for symptomatic primary hyperparathyroidism in older adults. Quality improvement efforts, rooted in equitable care, should be undertaken to increase access to parathyroidectomy for this disease.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest Disclosures:
The authors have no conflicts of interest to report.
Figures
References
-
- Lal G, Clark O. Thyroid, Parathyroid, and Adrenal. In: Schwartz’s Principles of Surgery. 11th ed. New York: McGraw-Hill; 2019:1663–1665.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
