

Integrated omics endotyping of infants with respiratory syncytial virus bronchiolitis and risk of childhood asthma
- PMID: 34127671
- PMCID: PMC8203688
- DOI: 10.1038/s41467-021-23859-6
Integrated omics endotyping of infants with respiratory syncytial virus bronchiolitis and risk of childhood asthma
Abstract
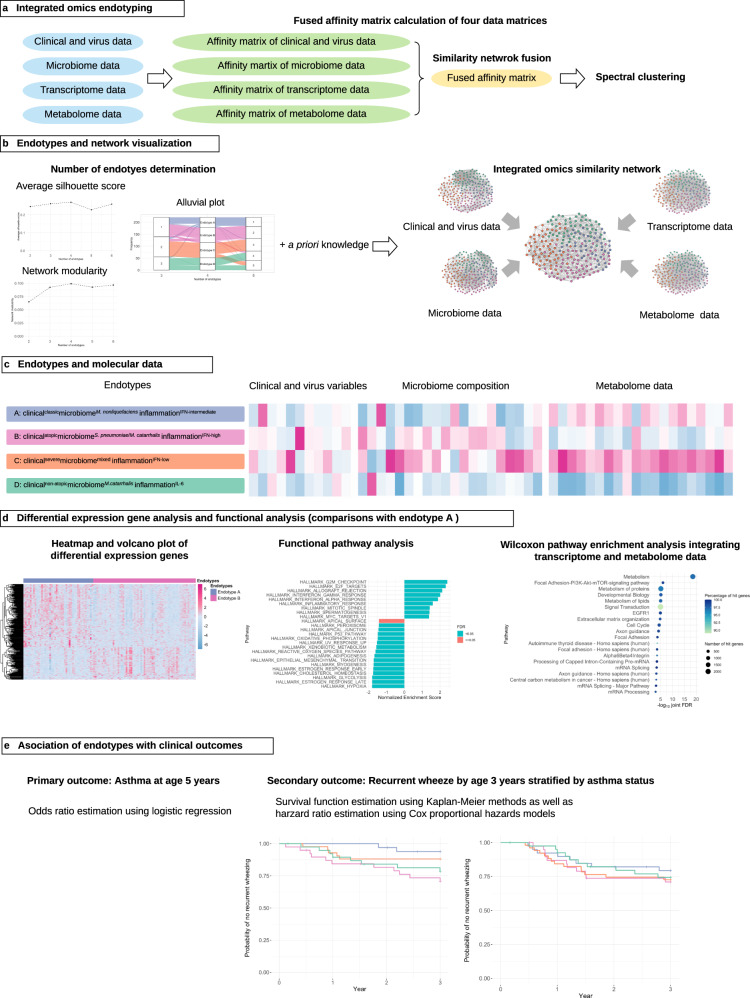
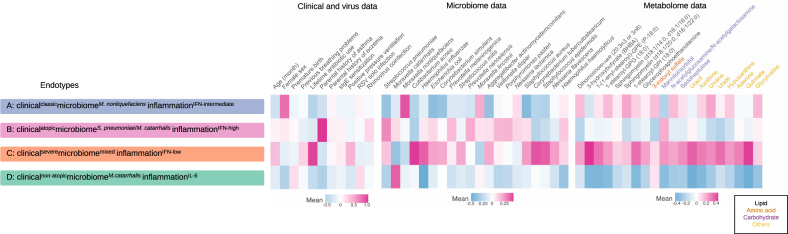
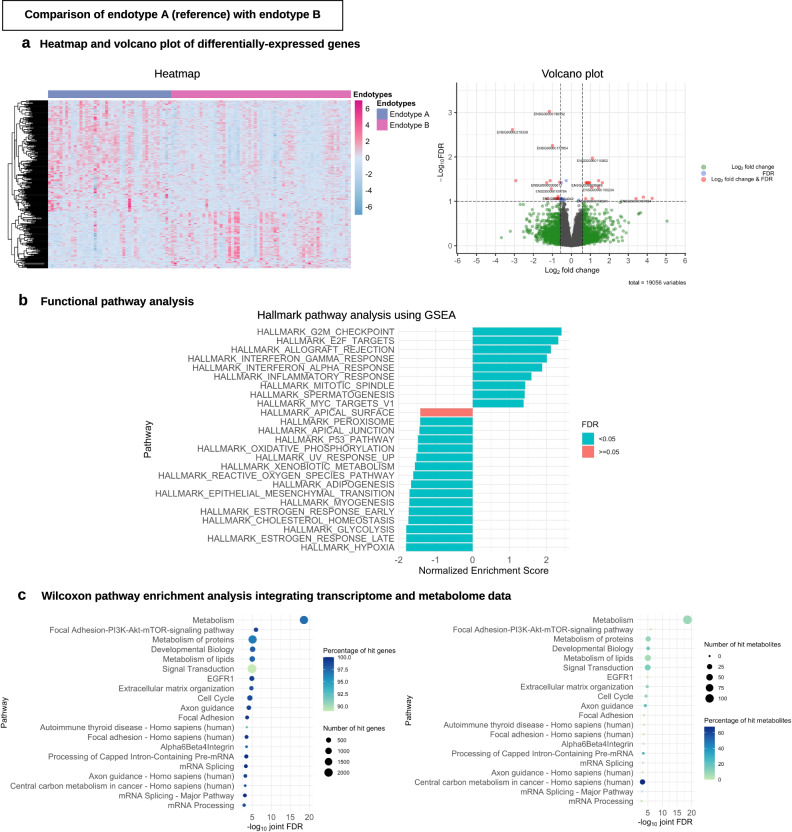
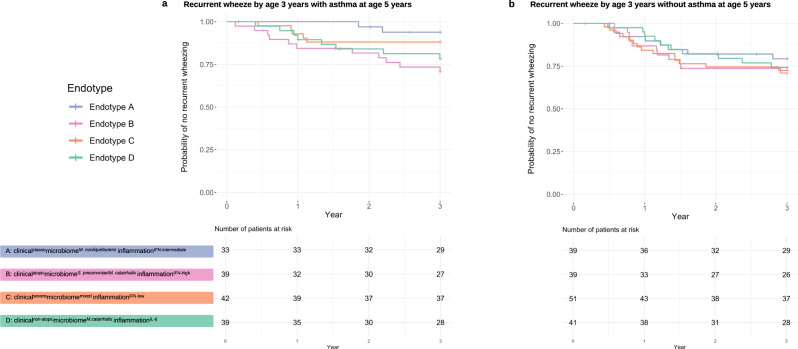
Respiratory syncytial virus (RSV) bronchiolitis is not only the leading cause of hospitalization in U.S. infants, but also a major risk factor for asthma development. While emerging evidence suggests clinical heterogeneity within RSV bronchiolitis, little is known about its biologically-distinct endotypes. Here, we integrated clinical, virus, airway microbiome (species-level), transcriptome, and metabolome data of 221 infants hospitalized with RSV bronchiolitis in a multicentre prospective cohort study. We identified four biologically- and clinically-meaningful endotypes: A) clinicalclassicmicrobiomeM. nonliquefaciensinflammationIFN-intermediate, B) clinicalatopicmicrobiomeS. pneumoniae/M. catarrhalisinflammationIFN-high, C) clinicalseveremicrobiomemixedinflammationIFN-low, and D) clinicalnon-atopicmicrobiomeM.catarrhalisinflammationIL-6. Particularly, compared with endotype A infants, endotype B infants-who are characterized by a high proportion of IgE sensitization and rhinovirus coinfection, S. pneumoniae/M. catarrhalis codominance, and high IFN-α and -γ response-had a significantly higher risk for developing asthma (9% vs. 38%; OR, 6.00: 95%CI, 2.08-21.9; P = 0.002). Our findings provide an evidence base for the early identification of high-risk children during a critical period of airway development.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
