

Association between aphasia severity and brain network alterations after stroke assessed using the electroencephalographic phase synchrony index
- PMID: 34127750
- PMCID: PMC8203681
- DOI: 10.1038/s41598-021-91978-7
Association between aphasia severity and brain network alterations after stroke assessed using the electroencephalographic phase synchrony index
Abstract
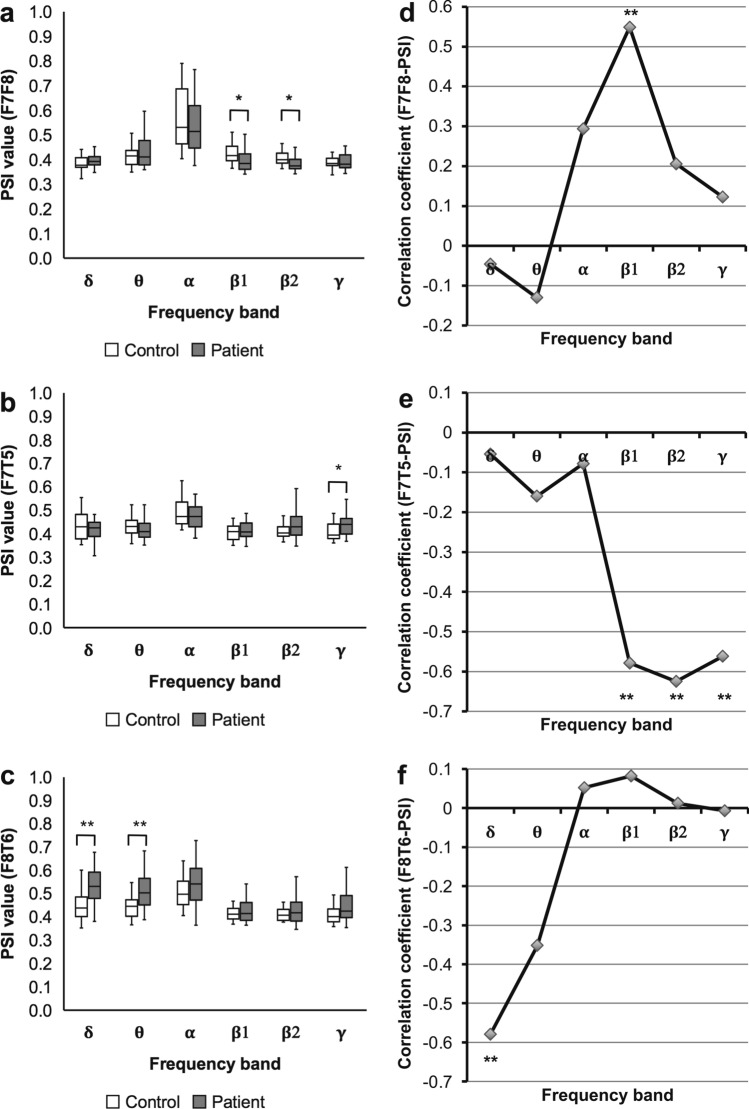
Electroencephalographic synchrony can help assess brain network status; however, its usefulness has not yet been fully proven. We developed a clinically feasible method that combines the phase synchrony index (PSI) with resting-state 19-channel electroencephalography (EEG) to evaluate post-stroke motor impairment. In this study, we investigated whether our method could be applied to aphasia, a common post-stroke cognitive impairment. This study included 31 patients with subacute aphasia and 24 healthy controls. We assessed the expressive function of patients and calculated the PSIs of three motor language-related regions: frontofrontal, left frontotemporal, and right frontotemporal. Then, we evaluated post-stroke network alterations by comparing PSIs of the patients and controls and by analyzing the correlations between PSIs and aphasia scores. The frontofrontal PSI (beta band) was lower in patients than in controls and positively correlated with aphasia scores, whereas the right frontotemporal PSI (delta band) was higher in patients than in controls and negatively correlated with aphasia scores. Evaluation of artifacts suggests that this association is attributed to true synchrony rather than spurious synchrony. These findings suggest that post-stroke aphasia is associated with alternations of two different networks and point to the usefulness of EEG PSI in understanding the pathophysiology of aphasia.
Conflict of interest statement
K. K. has a patent (JP6142354) issued to RIKEN and two patents (US14/770,047 and JPA2015-166281) pending to be issued to RIKEN. Y. U. has a patent (JPA2015-166281) pending to be issued to RIKEN. T. K., N. H., M. H., H. Y., H. F., M. N., H. M., and I. M. declare that they have no conflicts of interest to disclose.
Figures






References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
