

CD177, a specific marker of neutrophil activation, is associated with coronavirus disease 2019 severity and death
- PMID: 34127958
- PMCID: PMC8189740
- DOI: 10.1016/j.isci.2021.102711
CD177, a specific marker of neutrophil activation, is associated with coronavirus disease 2019 severity and death
Erratum in
-
Erratum: CD177, a specific marker of neutrophil activation, is associated with coronavirus disease 2019 severity and death.iScience. 2022 Dec 24;26(1):105715. doi: 10.1016/j.isci.2022.105715. eCollection 2023 Jan 20. iScience. 2022. PMID: 36590178 Free PMC article.
Abstract
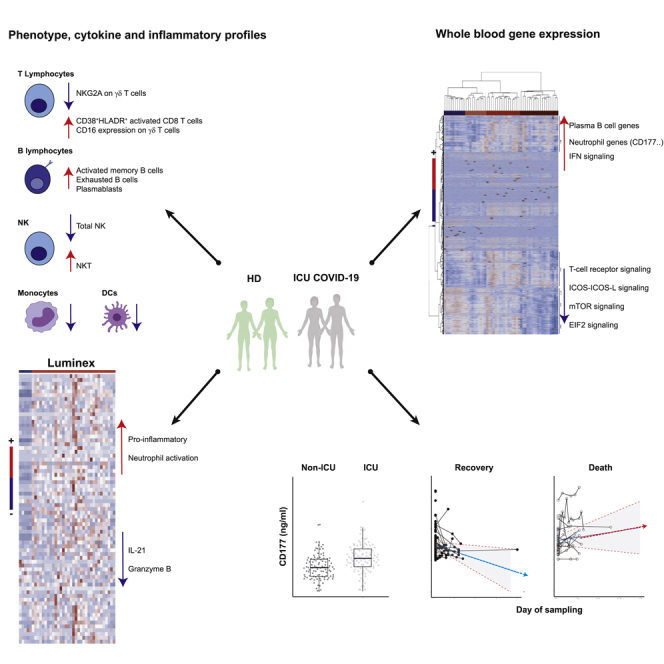
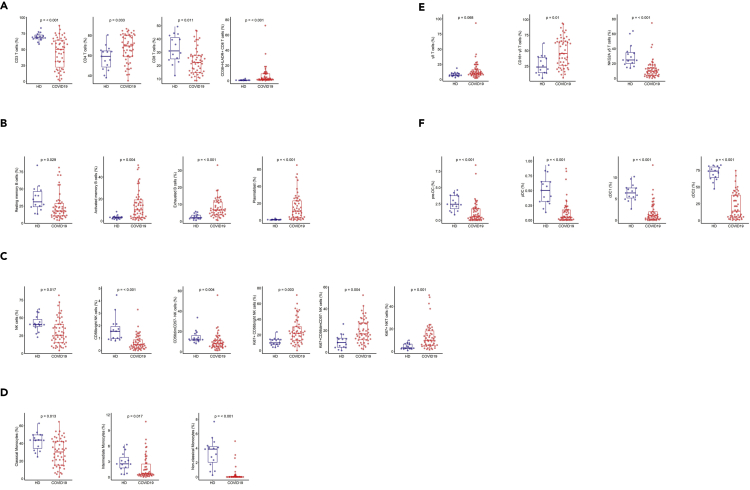
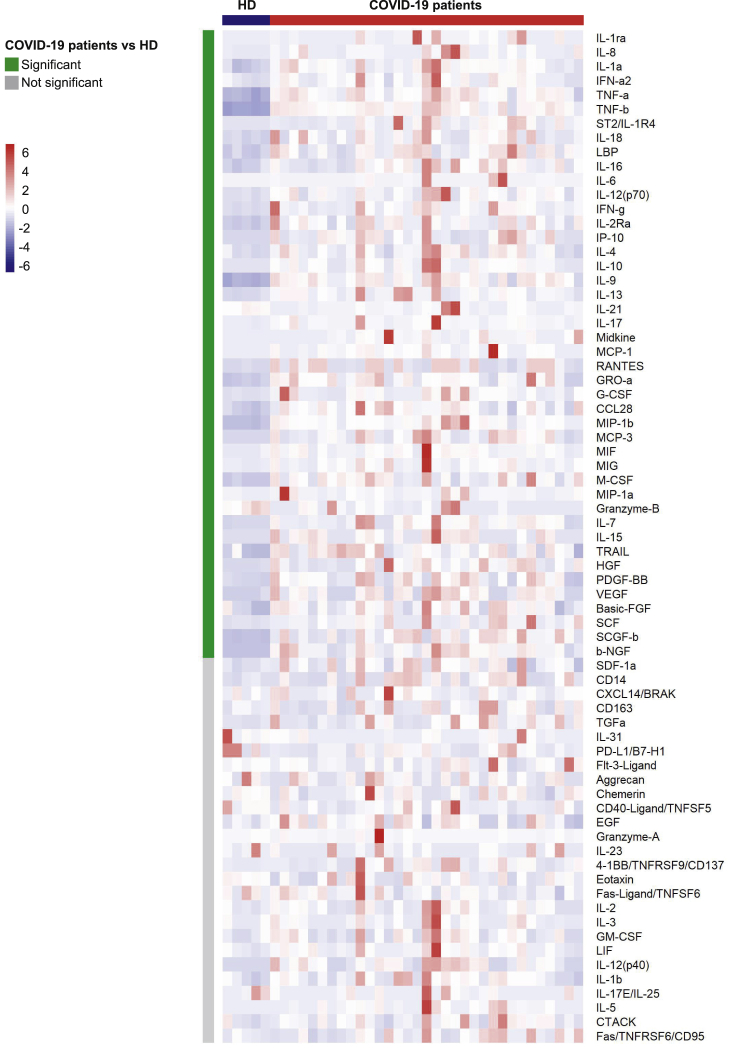
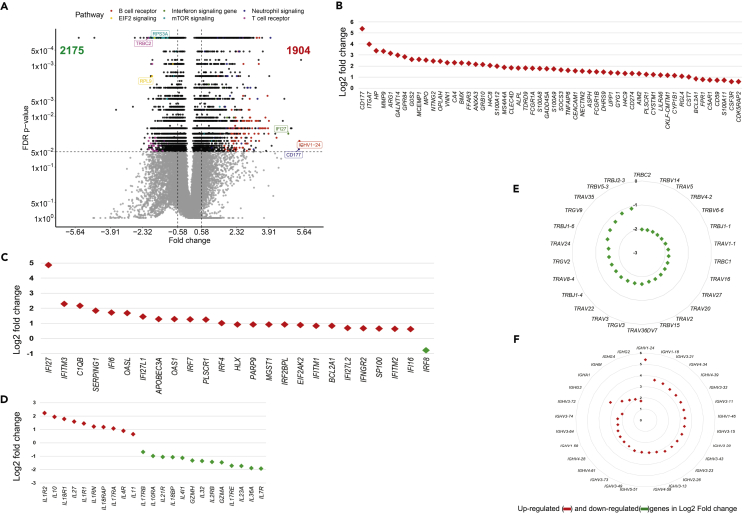
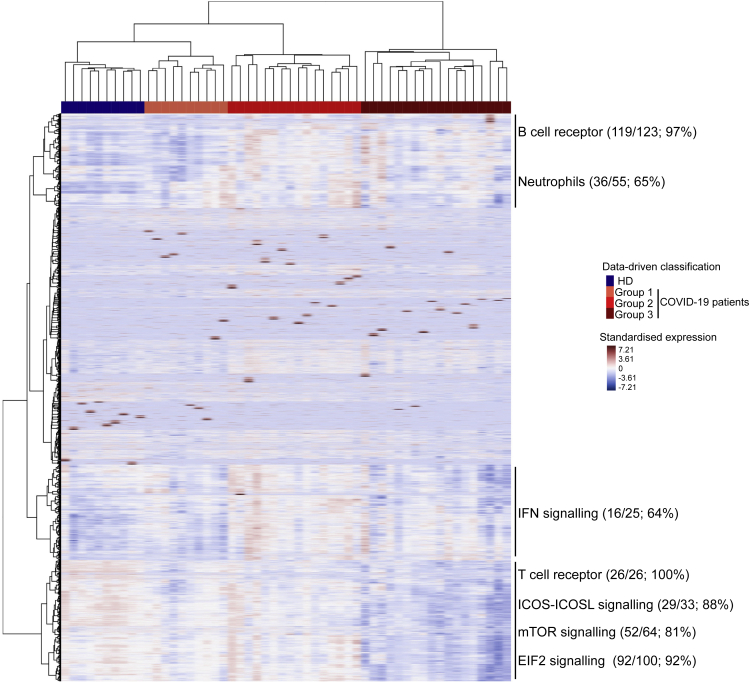
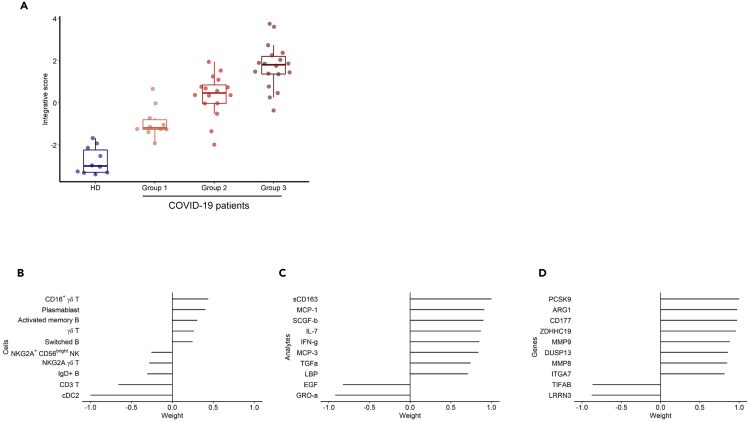
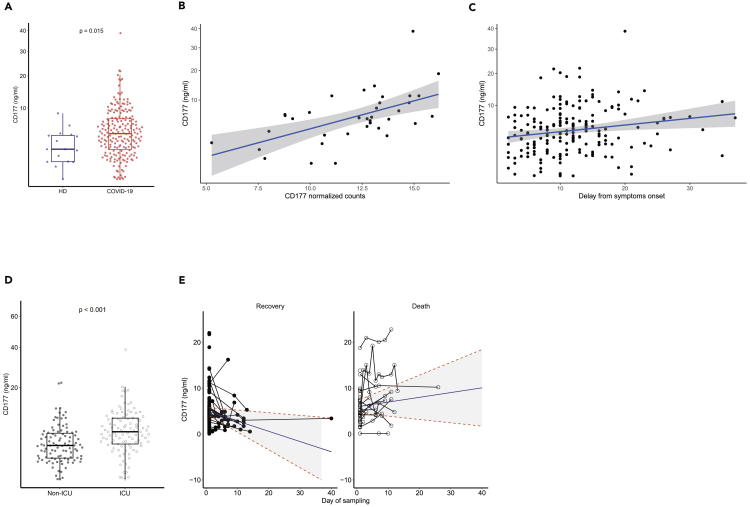
The identification of patients with coronavirus disease 2019 and high risk of severe disease is a challenge in routine care. We performed cell phenotypic, serum, and RNA sequencing gene expression analyses in severe hospitalized patients (n = 61). Relative to healthy donors, results showed abnormalities of 27 cell populations and an elevation of 42 cytokines, neutrophil chemo-attractants, and inflammatory components in patients. Supervised and unsupervised analyses revealed a high abundance of CD177, a specific neutrophil activation marker, contributing to the clustering of severe patients. Gene abundance correlated with high serum levels of CD177 in severe patients. Higher levels were confirmed in a second cohort and in intensive care unit (ICU) than non-ICU patients (P < 0.001). Longitudinal measurements discriminated between patients with the worst prognosis, leading to death, and those who recovered (P = 0.01). These results highlight neutrophil activation as a hallmark of severe disease and CD177 assessment as a reliable prognostic marker for routine care.
Keywords: immunology; virology.
© 2021 The Author(s).
Conflict of interest statement
None of the authors has any conflict of interest to declare.
Figures
References
-
- Augustin A., Kubo R.T., Sim G.K. Resident pulmonary lymphocytes expressing the gamma/delta T-cell receptor. Nature. 1989;340:239–241. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
