

A prospective study to establish the minimal clinically important difference of the Mini-BESTest in individuals with stroke
- PMID: 34128411
- PMCID: PMC8273365
- DOI: 10.1177/02692155211025131
A prospective study to establish the minimal clinically important difference of the Mini-BESTest in individuals with stroke
Abstract
Objective: To determine the minimal clinically important difference of the Mini-BESTest in individuals' post-stroke.
Design: Prospective cohort study.
Setting: Outpatient stroke rehabilitation.
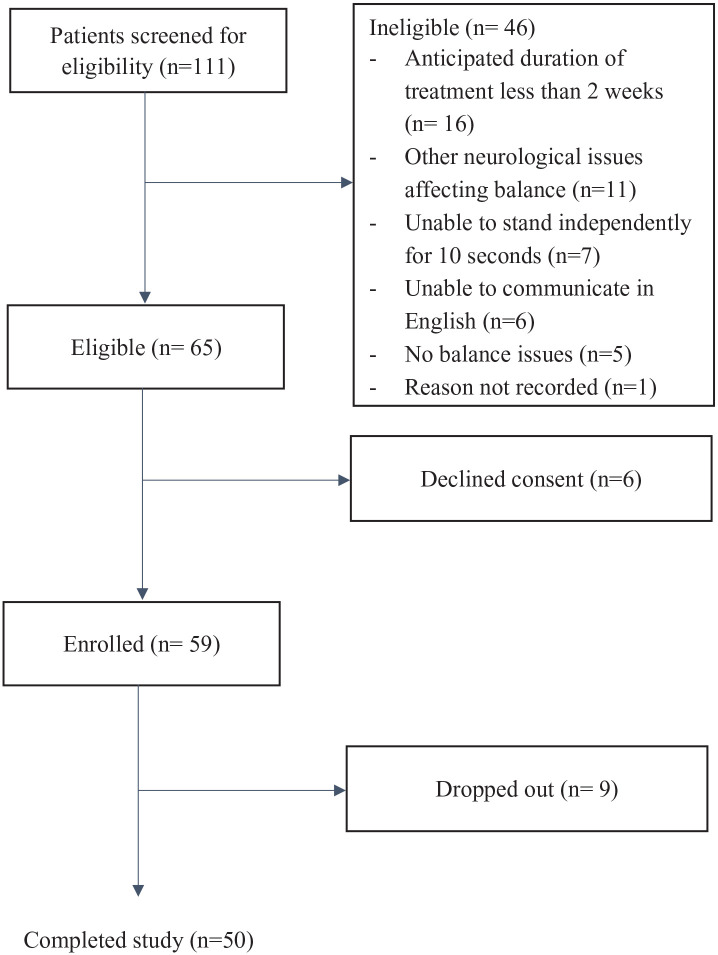
Subjects: Fifty outpatients with stroke with a mean (SD) age of 60.8 (9.4).
Intervention: Outpatients with stroke were assessed with the Mini-BESTest before and after a course of conventional rehabilitation. Rehabilitation sessions occurred one to two times/week for one hour and treatment duration was 1.3-42 weeks (mean (SD) = 17.4(10.6)).
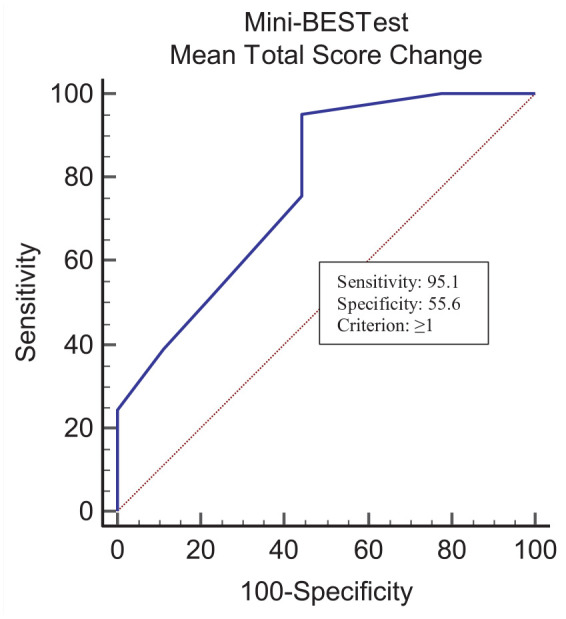
Main measures: We used a combination of anchor- and distribution-based approaches including a global rating of change in balance scale completed by physiotherapists and patients, the minimal detectable change with 95% confidence, and the optimal cut-point from receiver operating characteristic curves.
Results: The average (SD) Mini-BESTest score at admission was 18.2 (6.5) and 22.4 (5.2) at discharge (effect size: 0.7) (P = 0.001). Mean change scores on the Mini-BESTest for patient and physiotherapist ratings of small change were 4.2 and 4.3 points, and 4.7 and 5.3 points for substantial change, respectively. The minimal detectable change with 95% confidence for the Mini-BESTest was 3.2 points. The minimally clinical importance difference was determined to be 4 points for detecting small changes and 5 points for detecting substantial changes.
Conclusions: A change of 4-5 points on the Mini-BEST is required to be perceptible to clinicians and patients, and beyond measurement error. These values can be used to interpret changes in balance in stroke rehabilitation research and practice.
Keywords: MCID; Mini-BESTest; Stroke.
Conflict of interest statement
Figures
Comment in
-
Letter to the editor concerning the article: "A prospective study to establish the minimal clinically important difference of the Mini-BESTest in individuals with stroke".Clin Rehabil. 2022 Feb;36(2):283-285. doi: 10.1177/02692155211040733. Epub 2021 Sep 2. Clin Rehabil. 2022. PMID: 34472986 No abstract available.
Similar articles
-
The minimal clinically important difference of the mini-balance evaluation systems test in patients with early subacute stroke.Top Stroke Rehabil. 2023 Oct;30(7):672-680. doi: 10.1080/10749357.2022.2145759. Epub 2022 Nov 17. Top Stroke Rehabil. 2023. PMID: 36384452
-
Pooled Minimal Clinically Important Differences of the Mini-Balance Evaluation Systems Test in Patients With Early Subacute Stroke: A Multicenter Prospective Observational Study.Phys Ther. 2024 Apr 2;104(4):pzae017. doi: 10.1093/ptj/pzae017. Phys Ther. 2024. PMID: 38365440
-
Responsiveness and minimal clinically important difference of the Mini-BESTest in patients with Parkinson's disease.Gait Posture. 2020 Jul;80:14-19. doi: 10.1016/j.gaitpost.2020.05.004. Epub 2020 May 17. Gait Posture. 2020. PMID: 32464537
-
Comparison of reliability, validity, and responsiveness of the mini-BESTest and Berg Balance Scale in patients with balance disorders.Phys Ther. 2013 Feb;93(2):158-67. doi: 10.2522/ptj.20120171. Epub 2012 Sep 27. Phys Ther. 2013. PMID: 23023812
-
Psychometric Properties of Brief-Balance Evaluation Systems Test Among Multiple Populations: A Systematic Review and Meta-analysis.Arch Phys Med Rehabil. 2022 Jan;103(1):155-175.e2. doi: 10.1016/j.apmr.2021.04.013. Epub 2021 May 18. Arch Phys Med Rehabil. 2022. PMID: 34015349
Cited by
-
Effects of Home-Based Boxing Training on Trunk Performance, Balance, and Enjoyment of Patients With Chronic Stroke.Ann Rehabil Med. 2023 Feb;47(1):36-44. doi: 10.5535/arm.22127. Epub 2023 Jan 13. Ann Rehabil Med. 2023. PMID: 36635885 Free PMC article.
-
Responsiveness and Minimal Important Change of the Mini- and Brief-Balance Evaluation Systems Tests in People with Incomplete Cervical Spinal Cord Injury: A Prospective Cohort Study.Neurol Int. 2025 Mar 18;17(3):43. doi: 10.3390/neurolint17030043. Neurol Int. 2025. PMID: 40137465 Free PMC article.
-
Cutoff Point of Mini-Balance Evaluation Systems Test Scores for Elderly Estimated by Center of Pressure Measurements by Linear Regression and Decision Tree Classification.Life (Basel). 2022 Dec 17;12(12):2133. doi: 10.3390/life12122133. Life (Basel). 2022. PMID: 36556499 Free PMC article.
-
Effect of innovative vs. usual care physical therapy in subacute rehabilitation after stroke. A multicenter randomized controlled trial.Front Rehabil Sci. 2022 Sep 19;3:987601. doi: 10.3389/fresc.2022.987601. eCollection 2022. Front Rehabil Sci. 2022. PMID: 36407967 Free PMC article.
-
Minimal Clinically Important Difference of Scales Reported in Stroke Trials: A Review.Brain Sci. 2024 Jan 13;14(1):80. doi: 10.3390/brainsci14010080. Brain Sci. 2024. PMID: 38248295 Free PMC article. Review.
References
-
- Haley SM, Fragala-Pinkham MA. Interpreting change scores of tests and measures used in physical therapy. Phys Ther 2006; 86(5): 735–743. - PubMed
-
- Tsang CS, Liao LR, Chung RC, et al.. Psychometric properties of the mini-balance evaluation systems test (Mini-BESTest) in community-dwelling individuals with chronic stroke. Phys Ther 2013; 93(8): 1102–1115. - PubMed
-
- Terwee CB, Bot SD, de Boer MR, et al.. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol 2007; 60(1): 34–42. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
