

Acute Treatments for Episodic Migraine in Adults: A Systematic Review and Meta-analysis
- PMID: 34128998
- PMCID: PMC8207243
- DOI: 10.1001/jama.2021.7939
Acute Treatments for Episodic Migraine in Adults: A Systematic Review and Meta-analysis
Abstract
Importance: Migraine is common and can be associated with significant morbidity, and several treatment options exist for acute therapy.
Objective: To evaluate the benefits and harms associated with acute treatments for episodic migraine in adults.
Data sources: Multiple databases from database inception to February 24, 2021.
Study selection: Randomized clinical trials and systematic reviews that assessed effectiveness or harms of acute therapy for migraine attacks.
Data extraction and synthesis: Independent reviewers selected studies and extracted data. Meta-analysis was performed with the DerSimonian-Laird random-effects model with Hartung-Knapp-Sidik-Jonkman variance correction or by using a fixed-effect model based on the Mantel-Haenszel method if the number of studies was small.
Main outcomes and measures: The main outcomes included pain freedom, pain relief, sustained pain freedom, sustained pain relief, and adverse events. The strength of evidence (SOE) was graded with the Agency for Healthcare Research and Quality Methods Guide for Effectiveness and Comparative Effectiveness Reviews.
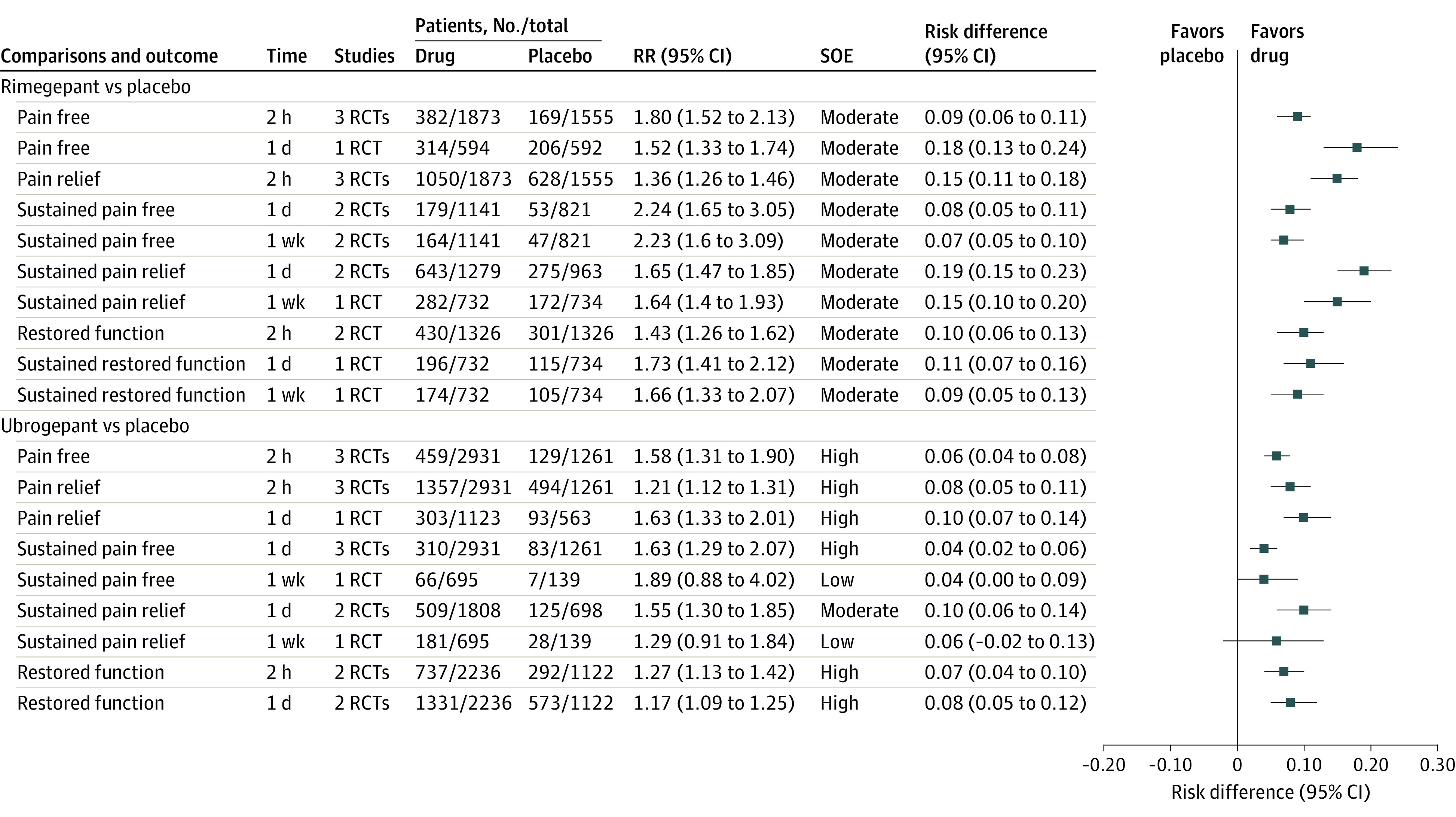
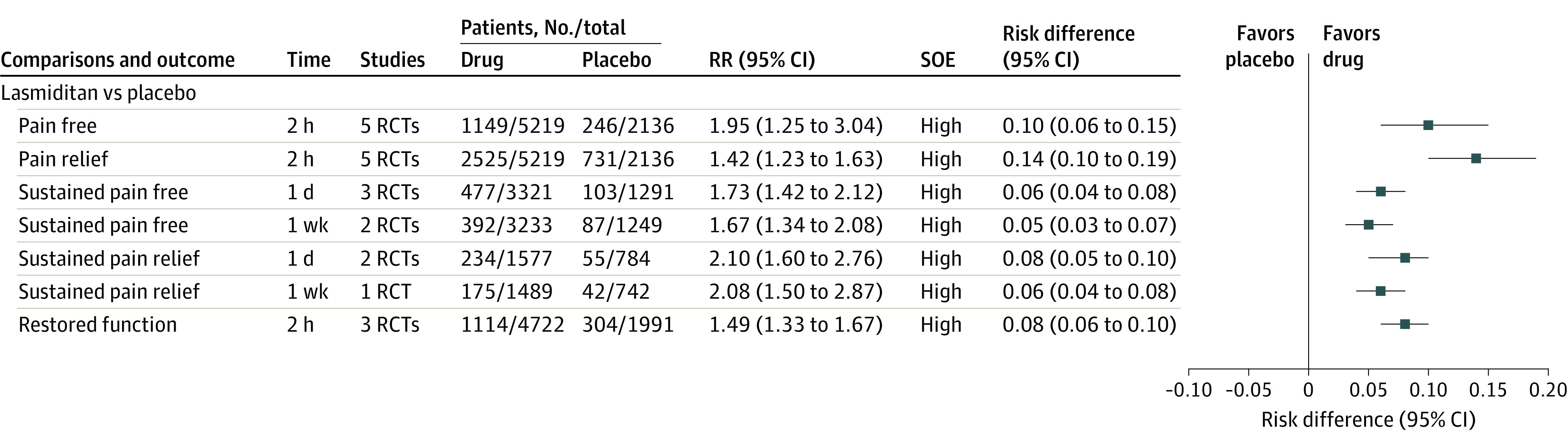
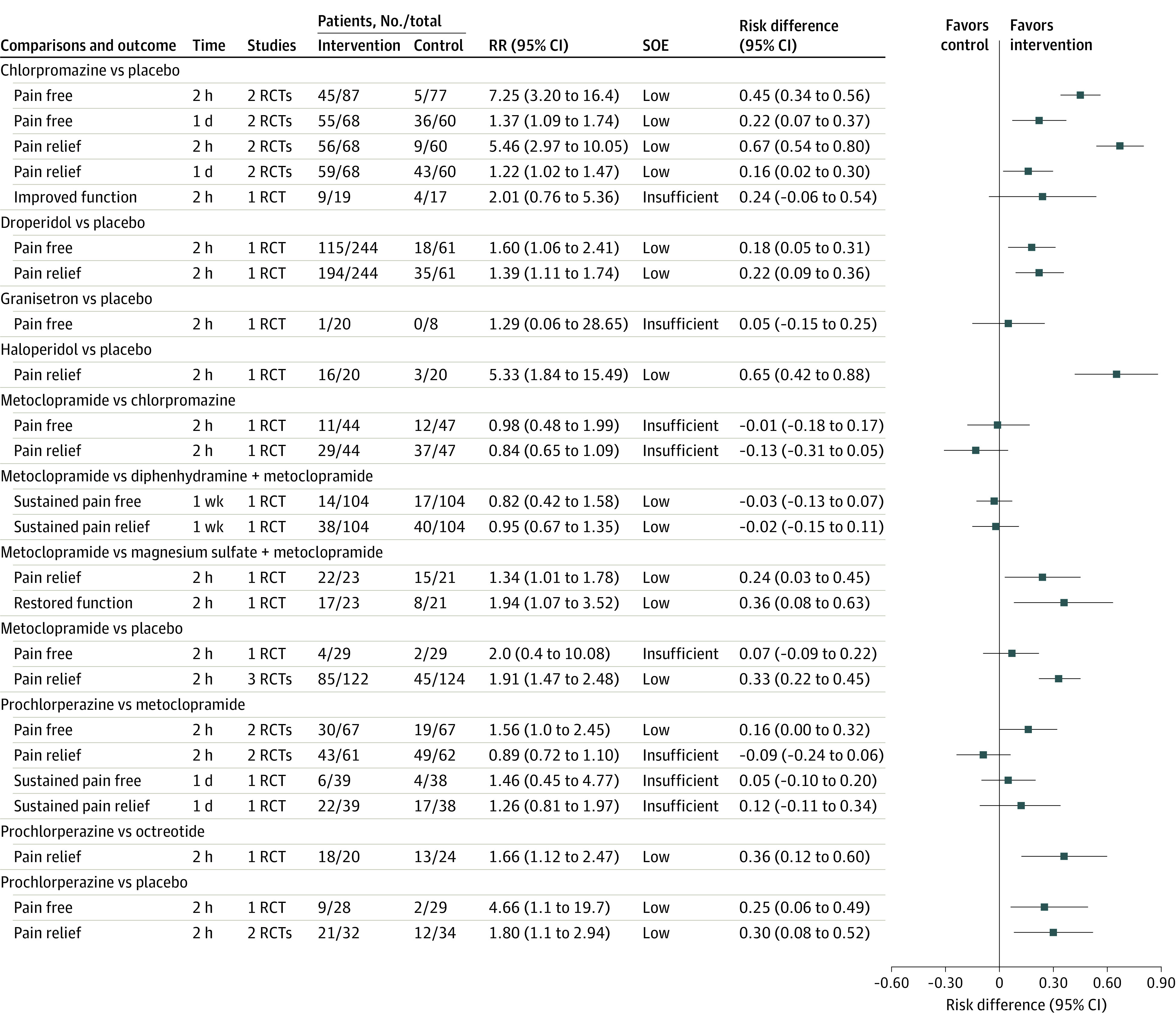
Findings: Evidence on triptans and nonsteroidal anti-inflammatory drugs was summarized from 15 systematic reviews. For other interventions, 115 randomized clinical trials with 28 803 patients were included. Compared with placebo, triptans and nonsteroidal anti-inflammatory drugs used individually were significantly associated with reduced pain at 2 hours and 1 day (moderate to high SOE) and increased risk of mild and transient adverse events. Compared with placebo, calcitonin gene-related peptide receptor antagonists (low to high SOE), lasmiditan (5-HT1F receptor agonist; high SOE), dihydroergotamine (moderate to high SOE), ergotamine plus caffeine (moderate SOE), acetaminophen (moderate SOE), antiemetics (low SOE), butorphanol (low SOE), and tramadol in combination with acetaminophen (low SOE) were significantly associated with pain reduction and increase in mild adverse events. The findings for opioids were based on low or insufficient SOE. Several nonpharmacologic treatments were significantly associated with improved pain, including remote electrical neuromodulation (moderate SOE), transcranial magnetic stimulation (low SOE), external trigeminal nerve stimulation (low SOE), and noninvasive vagus nerve stimulation (moderate SOE). No significant difference in adverse events was found between nonpharmacologic treatments and sham.
Conclusions and relevance: There are several acute treatments for migraine, with varying strength of supporting evidence. Use of triptans, nonsteroidal anti-inflammatory drugs, acetaminophen, dihydroergotamine, calcitonin gene-related peptide antagonists, lasmiditan, and some nonpharmacologic treatments was associated with improved pain and function. The evidence for many other interventions, including opioids, was limited.
Conflict of interest statement
Figures

Comment in
-
Acute Treatment for Migraine: Contemporary Treatments and Future Directions.JAMA. 2021 Jun 15;325(23):2346-2347. doi: 10.1001/jama.2021.7275. JAMA. 2021. PMID: 34129013 No abstract available.
-
Systematic Review and Meta-analysis of Acute Treatments for Episodic Migraine in Adults.JAMA. 2021 Oct 26;326(16):1636-1637. doi: 10.1001/jama.2021.14063. JAMA. 2021. PMID: 34698790 No abstract available.
-
Systematic Review and Meta-analysis of Acute Treatments for Episodic Migraine in Adults.JAMA. 2021 Oct 26;326(16):1636. doi: 10.1001/jama.2021.14060. JAMA. 2021. PMID: 34698791 No abstract available.
