

Clinical triage of patients on kidney replacement therapy presenting with COVID-19: an ERACODA registry analysis
- PMID: 34129039
- PMCID: PMC8420614
- DOI: 10.1093/ndt/gfab196
Clinical triage of patients on kidney replacement therapy presenting with COVID-19: an ERACODA registry analysis
Abstract
Background: Patients on kidney replacement therapy (KRT) are at very high risk of coronavirus disease 2019 (COVID-19). The triage pathway for KRT patients presenting to hospitals with varying severity of COVID-19 illness remains ill-defined. We studied the clinical characteristics of patients at initial and subsequent hospital presentations and the impact on patient outcomes.
Methods: The European Renal Association COVID-19 Database (ERACODA) was analysed for clinical and laboratory features of 1423 KRT patients with COVID-19 either hospitalized or non-hospitalized at initial triage and those re-presenting a second time. Predictors of outcomes (hospitalization, 28-day mortality) were then determined for all those not hospitalized at initial triage.
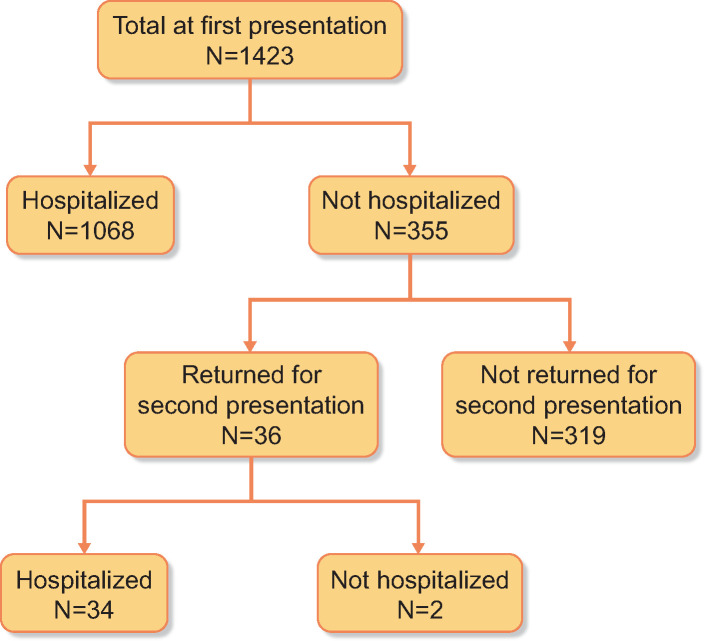
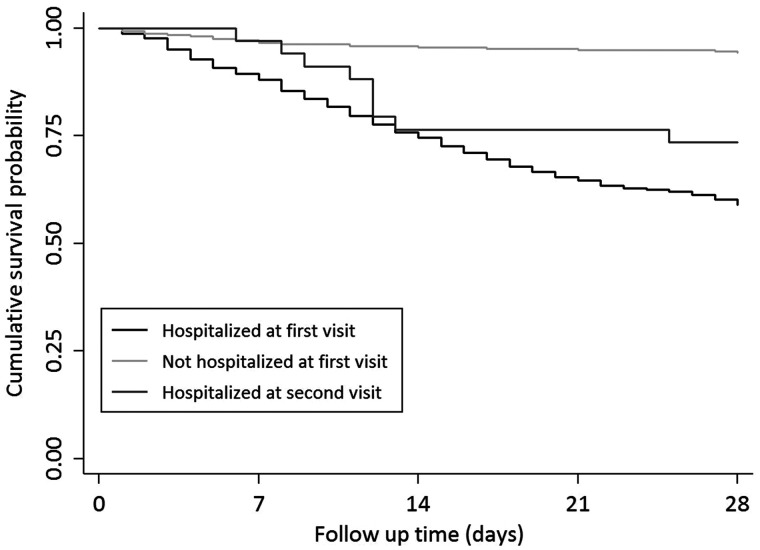
Results: Among 1423 KRT patients with COVID-19 [haemodialysis (HD), n = 1017; transplant, n = 406), 25% (n = 355) were not hospitalized at first presentation due to mild illness (30% HD, 13% transplant). Of the non-hospitalized patients, only 10% (n = 36) re-presented a second time, with a 5-day median interval between the two presentations (interquartile range 2-7 days). Patients who re-presented had worsening respiratory symptoms, a decrease in oxygen saturation (97% versus 90%) and an increase in C-reactive protein (26 versus 73 mg/L) and were older (72 vs 63 years) compared with those who did not return a second time. The 28-day mortality between early admission (at first presentation) and deferred admission (at second presentation) was not significantly different (29% versus 25%; P = 0.6). Older age, prior smoking history, higher clinical frailty score and self-reported shortness of breath at first presentation were identified as risk predictors of mortality when re-presenting after discharge at initial triage.
Conclusions: This study provides evidence that KRT patients with COVID-19 and mild illness can be managed effectively with supported outpatient care and with vigilance of respiratory symptoms, especially in those with risk factors for poor outcomes. Our findings support a risk-stratified clinical approach to admissions and discharges of KRT patients presenting with COVID-19 to aid clinical triage and optimize resource utilization during the ongoing pandemic.
Keywords: COVID-19; dialysis; kidney; mortality; second presentation; transplantation.
© The Author(s) 2021. Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
