

Cerebrovascular disease, neurodegeneration, and clinical phenotype in dementia with Lewy bodies
- PMID: 34130107
- PMCID: PMC8338792
- DOI: 10.1016/j.neurobiolaging.2021.04.029
Cerebrovascular disease, neurodegeneration, and clinical phenotype in dementia with Lewy bodies
Abstract
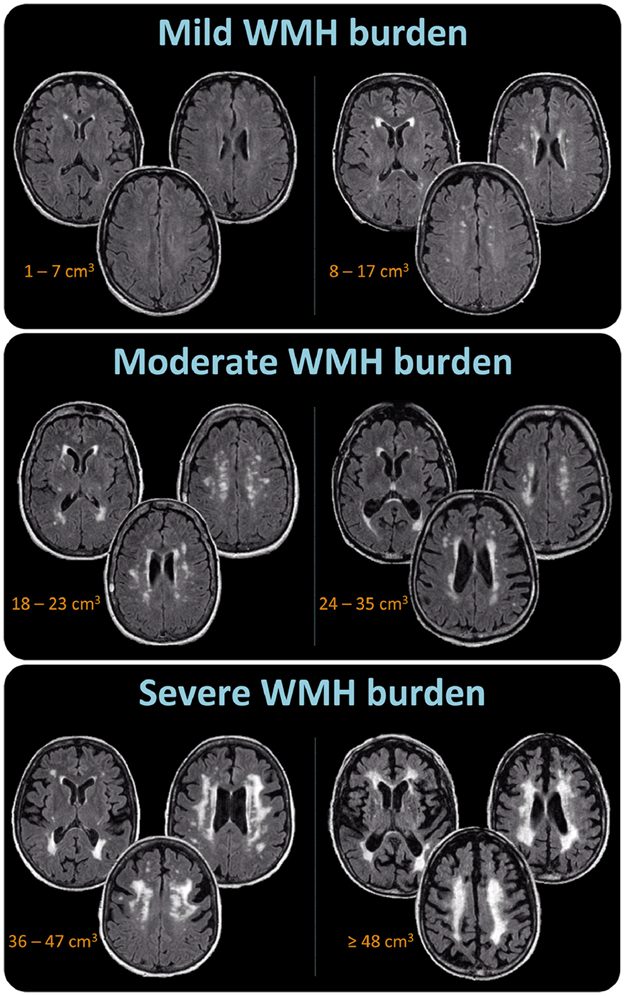
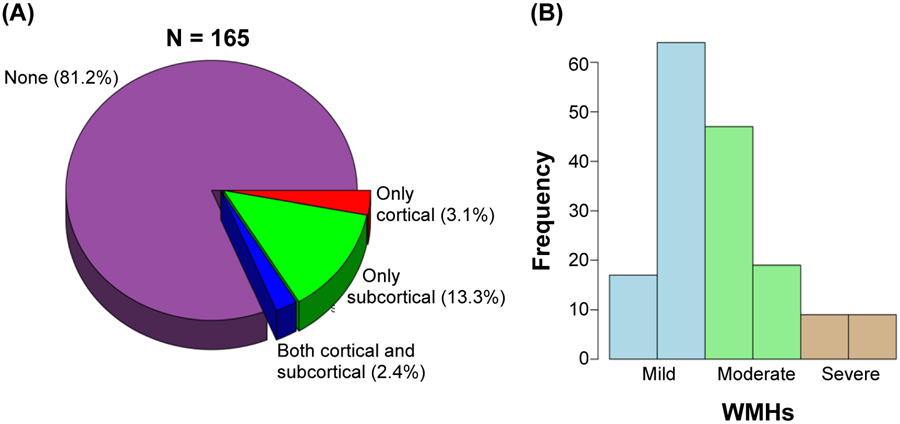
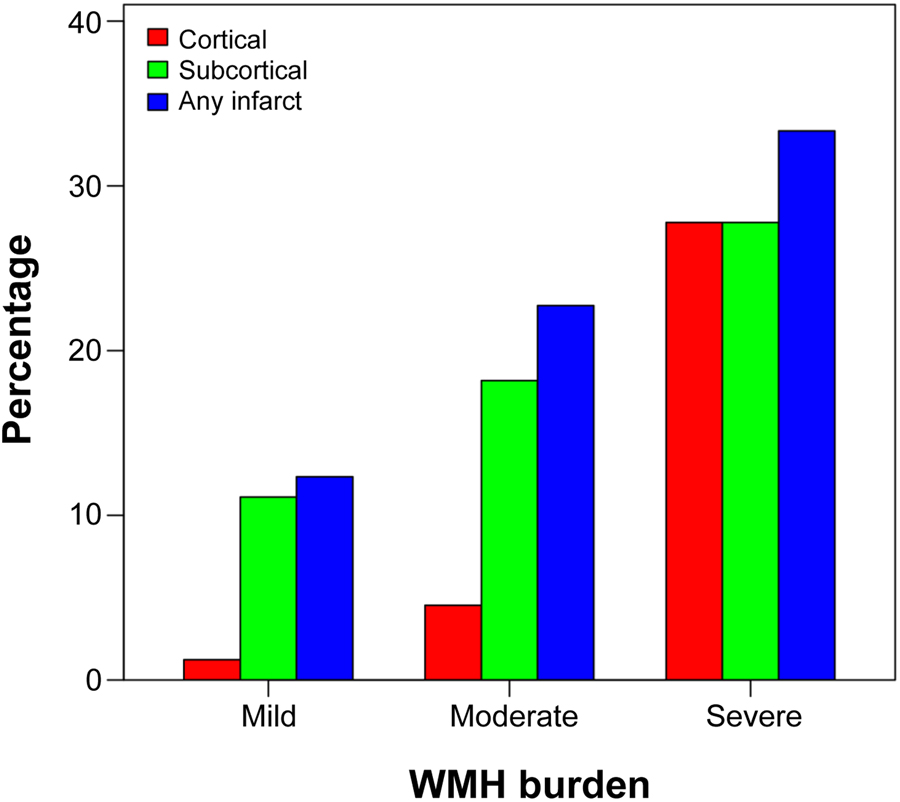
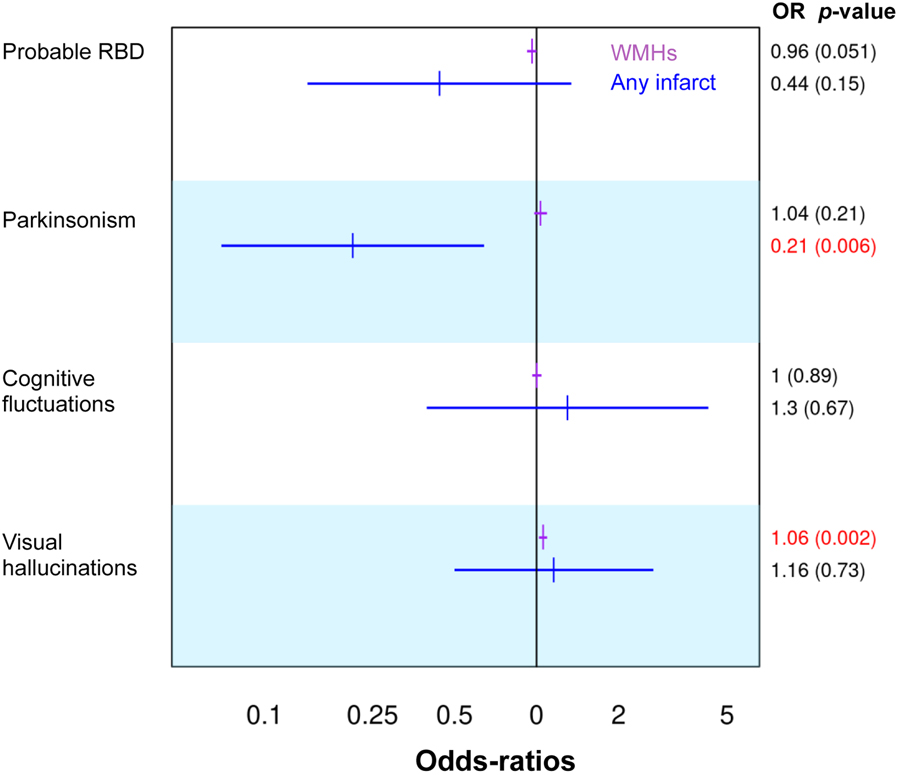
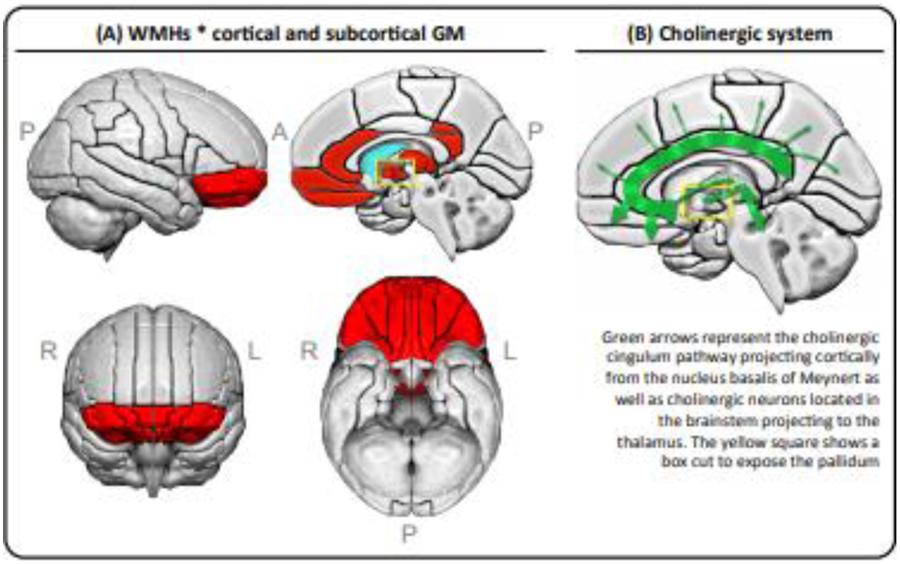
We investigated whether cerebrovascular disease contributes to neurodegeneration and clinical phenotype in dementia with Lewy bodies (DLB). Regional cortical thickness and subcortical gray matter volumes were estimated from structural magnetic resonance imaging (MRI) in 165 DLB patients. Cortical and subcortical infarcts were recorded and white matter hyperintensities (WMHs) were assessed. Subcortical only infarcts were more frequent (13.3%) than cortical only infarcts (3.1%) or both subcortical and cortical infarcts (2.4%). Infarcts, irrespective of type, were associated with WMHs. A higher WMH volume was associated with thinner orbitofrontal, retrosplenial, and posterior cingulate cortices, smaller thalamus and pallidum, and larger caudate volume. A higher WMH volume was associated with the presence of visual hallucinations and lower global cognitive performance, and tended to be associated with the absence of probable rapid eye movement sleep behavior disorder. Presence of infarcts was associated with the absence of parkinsonism. We conclude that cerebrovascular disease is associated with gray matter neurodegeneration in patients with probable DLB, which may have implications for the multifactorial treatment of probable DLB.
Keywords: Cerebrovascular disease; Dementia with Lewy bodies (DLB); Magnetic resonance imaging; Neurodegeneration; White matter hyperintensities; infarcts.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
CONFLICTS OF INTEREST
D Ferreira, SA Przybelski, TG Lesnick, AW Lemstra, Z Nedelska, CG Schwarz, H Botha, ML Senjem, JA Fields, DS Knopman, R Savica, NR Graff-Radford, RC Petersen, J Hort, K Oppedal, and E Westman report no disclosures relevant to the manuscript. J Graff-Radford receives research support from NIH. T Ferman receives funding from the Mangurian Foundation for Lewy body research and NIH. VJ Lowe serves as a consultant for AVID Radiopharmaceuticals, Bayer Schering Pharma, Eisai Inc, Philips Molecular Imaging, and Piramal Imaging and receives research support from GE Healthcare, Siemens Molecular Imaging, AVID Radiopharmaceuticals, the NIH (NIA, NCI), and the MN Partnership for Biotechnology and Medical Genomics. CR Jack has consulted for Lily, serves on an independent data monitoring board for Roche, and as a speaker for Eisai, but he receives no personal compensation from any commercial entity. He receives research support from NIH and the Alexander Family Alzheimer’s Disease Research Professorship of the Mayo Clinic. F Blanc, has served as national coordinator and principal investigator for clinical trials sponsored by Biogen, Roche, Axovant and Eisai. BF Boeve has served as an investigator for clinical trials sponsored by Biogen and Alector. He receives royalties from the publication of a book entitled Behavioral Neurology Of Dementia (Cambridge Medicine, 2017). He serves on the Scientific Advisory Board of the Tau Consortium. He receives research support from NIH, the Mayo Clinic Dorothy and Harry T. Mangurian Jr. Lewy Body Dementia Program and the Little Family Foundation. D Aarsland has received research support and/or honoraria from AstraZeneca, H. Lundbeck, Novartis Pharmaceuticals and GE Health, and served as paid consultant for H. Lundbeck, Eisai and Evonik. K Kantarci serves on the data safety monitoring board for Takeda Global Research and Development Center, Inc.; receives research support from Avid Radiopharmaceuticals and Eli Lilly, and receives funding from NIH and Alzheimer’s Drug Discovery Foundation.
Figures
References
-
- AASM, 2005. International Classification of Sleep Disorders–2: Diagnostic and Coding Manual. American Academy of Sleep Medicine, Chicago.
-
- Abdelnour C, Ferreira D, Oppedal K, Cavallin L, Bousiges O, Olof L, Hort J, Nedelska Z, Padovani A, Pilotto A, Bonanni L, Kramberger MG, Boada M, Westman E, Pagonabarraga J, Kulisevsky J, Blanc F, Aarsland D The combined effect of amyloid-β and tau biomarkers on brain atrophy in dementia with Lewy bodies. Neuroimage Clin 2020;27:102333. doi: 10.1016/j.nicl.2020.102333. - DOI - PMC - PubMed
