

Dynamic Fixation Techniques for the Prevention of Adjacent Segment Disease: A Retrospective Controlled Study
- PMID: 34130381
- PMCID: PMC9260399
- DOI: 10.31616/asj.2020.0585
Dynamic Fixation Techniques for the Prevention of Adjacent Segment Disease: A Retrospective Controlled Study
Abstract
Study design: Retrospective, controlled study.
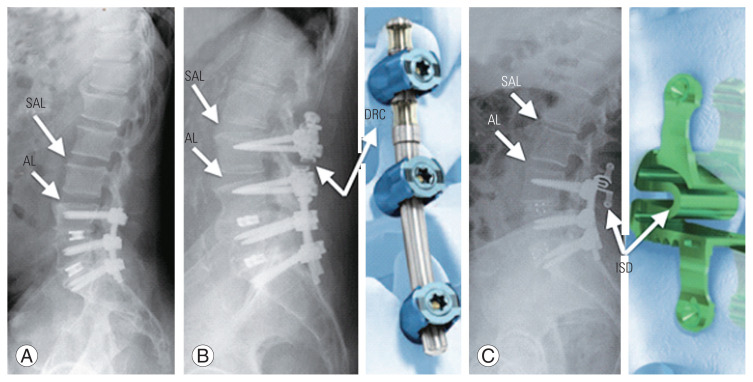
Purpose: Dynamic fixation (topping-off technique) adjacent to a transforaminal lumbar interbody fusion (TLIF) level was developed to reduce the risk of adjacent segment disease (ASDi). This study was designed to compare the clinical and radiological outcomes between patients who underwent circumferential lumbar fusion (CLF) without the topping-off technique, CLF with dynamic rod constructs (DRC), and CLF with interspinous device (ISD).
Overview of literature: Lumbar fusion can result in the re-distribution of stress, increased mobility, and increased intradiscal pressure at adjacent levels, ultimately leading to adjacent segment degeneration (ASDe) and ASDi. Dynamic fixation techniques (topping-off techniques) adjacent to vertebral fusion have been developed to reduce the risk of ASDe and ASDi because they provide a transitional zone between a caudal rigid fused segment and cephalad-mobile unfused levels.
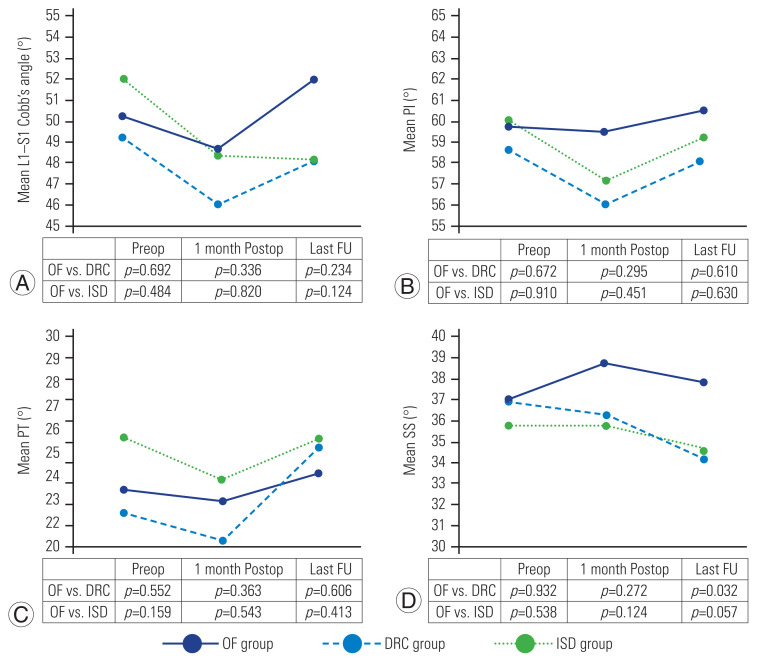
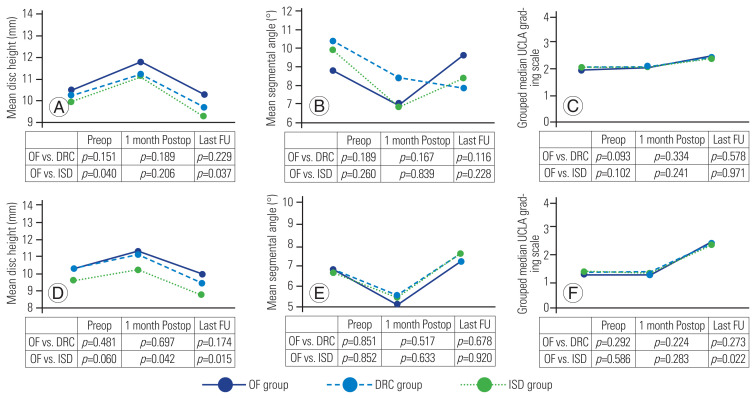
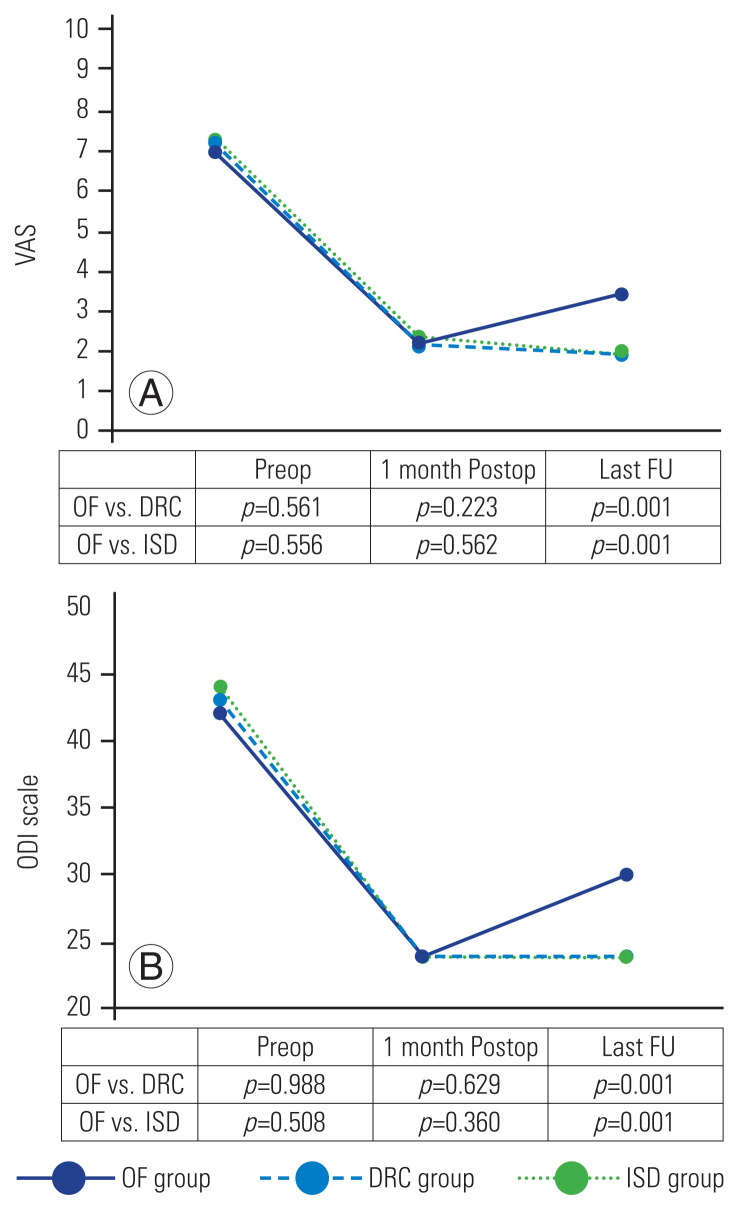
Methods: A single-center, retrospective, controlled study was designed, including all patients who underwent CLF due to degenerative lumbar spinal disease in Hospital Clinic of Barcelona between 2012 and 2018. Three groups of patients were evaluated as per the type of topping-off technique used: CLF alone group, DRC group, and ISD group. Clinical and radiological outcomes were evaluated.
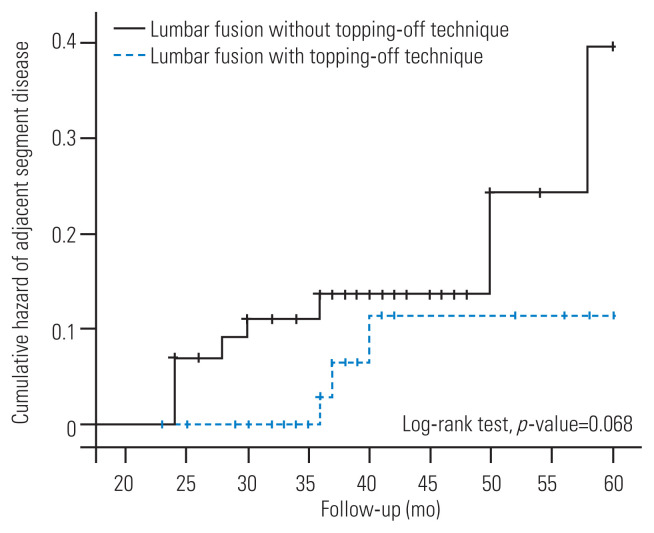
Results: A total of 117 patients were enrolled in the study. Sixty patients (51.3%) underwent CLF without dynamic stabilization, 24 (20.5%) were treated with DRC as topping-off technique, and 33 (28.5%) were treated with an ISD. A total of 12 patients (20.0%) in the CLF alone group showed ASDi at the final follow-up, compared to 1 (4.2%) in the DRC group (p=0.097) and 2 (6.1%) in the ISD group (p=0.127). The Cox regression model identified a significantly decreased risk of ASDi when a topping-off technique (DRC or ISD) was used (hazard ratio, 0.154; 95% confidence interval, 0.31-0.77).
Conclusions: Dynamic fixation adjacent to CLF was a safe and efficient procedure associated with improved clinical outcomes in patients with lumbar spine degenerative disease.
Keywords: Adjacent segment degeneration; Lumbar instrumentation; Lumbosacral region; Posterolateral fusion.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Helgeson MD, Bevevino AJ, Hilibrand AS. Update on the evidence for adjacent segment degeneration and disease. Spine J. 2013;13:342–51. - PubMed
-
- Ghiselli G, Wang JC, Hsu WK, Dawson EG. L5–S1 segment survivorship and clinical outcome analysis after L4–L5 isolated fusion. Spine (Phila Pa 1976) 2003;28:1275–80. - PubMed
-
- Pfirrmann CW, Metzdorf A, Zanetti M, Hodler J, Boos N. Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine (Phila Pa 1976) 2001;26:1873–8. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
