

An observational claims data analysis on the risk of maternal chronic kidney disease after preterm delivery and preeclampsia
- PMID: 34131246
- PMCID: PMC8206322
- DOI: 10.1038/s41598-021-92078-2
An observational claims data analysis on the risk of maternal chronic kidney disease after preterm delivery and preeclampsia
Abstract
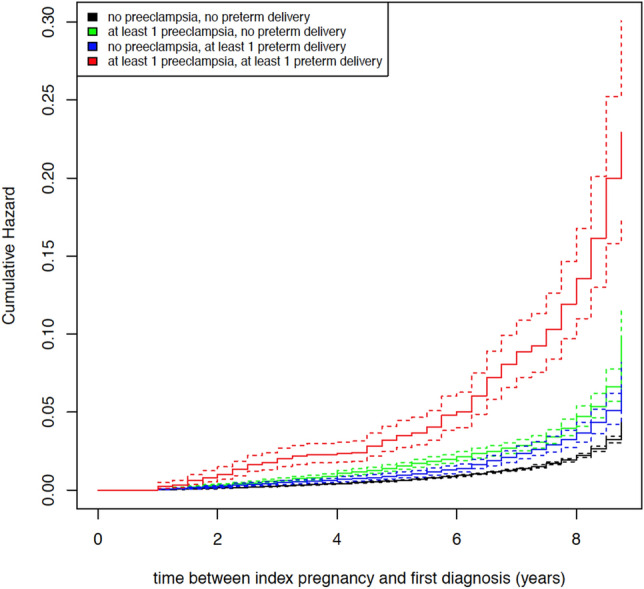
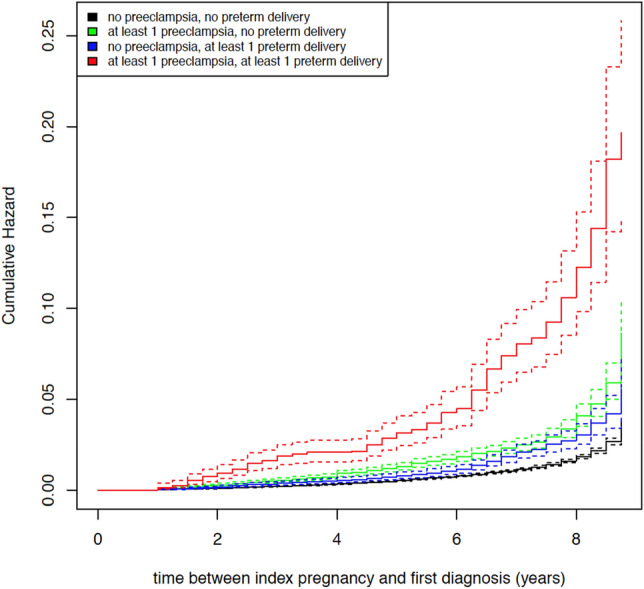
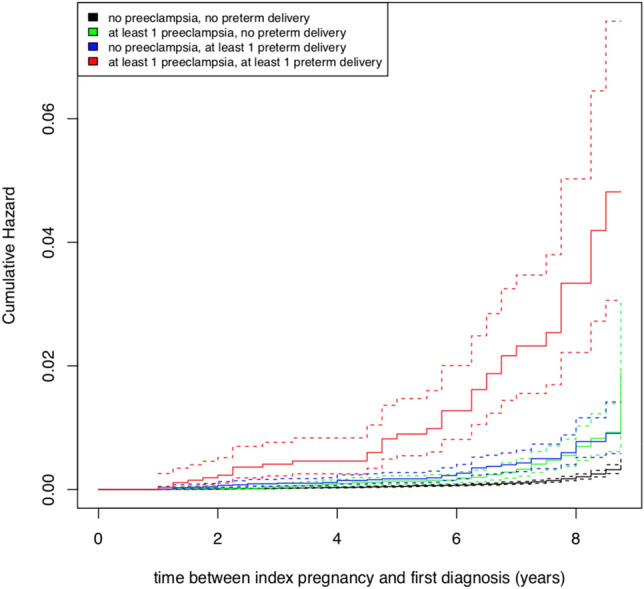
Women with complications of pregnancy such as preeclampsia and preterm birth are at risk for adverse long-term outcomes, including an increased future risk of chronic kidney disease (CKD) and end-stage kidney disease (ESKD). This observational cohort study aimed to examine the risk of CKD after preterm delivery and preeclampsia in a large obstetric cohort in Germany, taking into account preexisting comorbidities, potential confounders, and the severity of CKD. Statutory claims data of the AOK Baden-Wuerttemberg were used to identify women with singleton live births between 2010 and 2017. Women with preexisting conditions including CKD, ESKD, and kidney replacement therapy (KRT) were excluded. Preterm delivery (< 37 gestational weeks) was the main exposure of interest; preeclampsia was investigated as secondary exposure. The main outcome was a newly recorded diagnosis of CKD in the claims database. Data were analyzed using Cox proportional hazard regression models. The time-dependent occurrence of CKD was analyzed for four strata, i.e., births with (i) neither an exposure of preterm delivery nor an exposure of preeclampsia, (ii) no exposure of preterm delivery but exposure of at least one preeclampsia, (iii) an exposure of at least one preterm delivery but no exposure of preeclampsia, or (iv) joint exposure of preterm delivery and preeclampsia. Risk stratification also included different CKD stages. Adjustments were made for confounding factors, such as maternal age, diabetes, obesity, and dyslipidemia. The cohort consisted of 193,152 women with 257,481 singleton live births. Mean observation time was 5.44 years. In total, there were 16,948 preterm deliveries (6.58%) and 14,448 births with at least one prior diagnosis of preeclampsia (5.61%). With a mean age of 30.51 years, 1,821 women developed any form of CKD. Compared to women with no risk exposure, women with a history of at least one preterm delivery (HR = 1.789) and women with a history of at least one preeclampsia (HR = 1.784) had an increased risk for any subsequent CKD. The highest risk for CKD was found for women with a joint exposure of preterm delivery and preeclampsia (HR = 5.227). These effects were the same in magnitude only for the outcome of mild to moderate CKD, but strongly increased for the outcome of severe CKD (HR = 11.90). Preterm delivery and preeclampsia were identified as independent risk factors for all CKD stages. A joint exposure or preterm birth and preeclampsia was associated with an excessive maternal risk burden for CKD in the first decade after pregnancy. Since consequent follow-up policies have not been defined yet, these results will help guide long-term surveillance for early detection and prevention of kidney disease, especially for women affected by both conditions.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Hypertensive disorders of pregnancy and the risk of chronic kidney disease: A Swedish registry-based cohort study.PLoS Med. 2020 Aug 14;17(8):e1003255. doi: 10.1371/journal.pmed.1003255. eCollection 2020 Aug. PLoS Med. 2020. PMID: 32797043 Free PMC article.
-
Risk of long-term renal disease in women with a history of preterm delivery: a population-based cohort study.BMC Med. 2020 Apr 1;18(1):66. doi: 10.1186/s12916-020-01534-9. BMC Med. 2020. PMID: 32234061 Free PMC article.
-
Preeclampsia and risk of end stage kidney disease: A Swedish nationwide cohort study.PLoS Med. 2019 Jul 30;16(7):e1002875. doi: 10.1371/journal.pmed.1002875. eCollection 2019 Jul. PLoS Med. 2019. PMID: 31361741 Free PMC article.
-
Adverse Pregnancy Outcomes and Long-term Maternal Kidney Disease: A Systematic Review and Meta-analysis.JAMA Netw Open. 2020 Feb 5;3(2):e1920964. doi: 10.1001/jamanetworkopen.2019.20964. JAMA Netw Open. 2020. PMID: 32049292
-
Reflux nephropathy and the risk of preeclampsia and of other adverse pregnancy-related outcomes: a systematic review and meta-analysis of case series and reports in the new millennium.J Nephrol. 2018 Dec;31(6):833-846. doi: 10.1007/s40620-018-0515-1. Epub 2018 Jul 31. J Nephrol. 2018. PMID: 30066252
Cited by
-
Association between preterm delivery and the risk of maternal renal disease: A systematic review and meta‑analysis.Exp Ther Med. 2024 Jul 26;28(4):378. doi: 10.3892/etm.2024.12667. eCollection 2024 Oct. Exp Ther Med. 2024. PMID: 39113909 Free PMC article.
-
Assessing Severity and Need for Delivery in Early Onset Preeclampsia Before 32 Weeks of Gestation: a Delphi Consensus Procedure.Geburtshilfe Frauenheilkd. 2024 Aug 6;84(8):760-772. doi: 10.1055/a-2361-0563. eCollection 2024 Aug. Geburtshilfe Frauenheilkd. 2024. PMID: 39114380 Free PMC article.
-
Observational database study on preeclampsia and postpartum medical care up to 7.5 years after birth.Sci Rep. 2022 Dec 8;12(1):21230. doi: 10.1038/s41598-022-25596-2. Sci Rep. 2022. PMID: 36482054 Free PMC article.
-
Placental and Renal Pathways Underlying Pre-Eclampsia.Int J Mol Sci. 2024 Feb 27;25(5):2741. doi: 10.3390/ijms25052741. Int J Mol Sci. 2024. PMID: 38473987 Free PMC article. Review.
-
Heme oxygenase/carbon monoxide system affects the placenta and preeclampsia.Med Gas Res. 2025 Jun 1;15(2):276-287. doi: 10.4103/mgr.MEDGASRES-D-24-00081. Epub 2025 Jan 18. Med Gas Res. 2025. PMID: 39829164 Free PMC article. Review.
References
-
- World Health Organisation. Fact Sheet. Preterm Birth. Vol. 2020 (2018).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
