

Emerging therapeutic approaches for the treatment of NAFLD and type 2 diabetes mellitus
- PMID: 34131333
- PMCID: PMC8570106
- DOI: 10.1038/s41574-021-00507-z
Emerging therapeutic approaches for the treatment of NAFLD and type 2 diabetes mellitus
Abstract
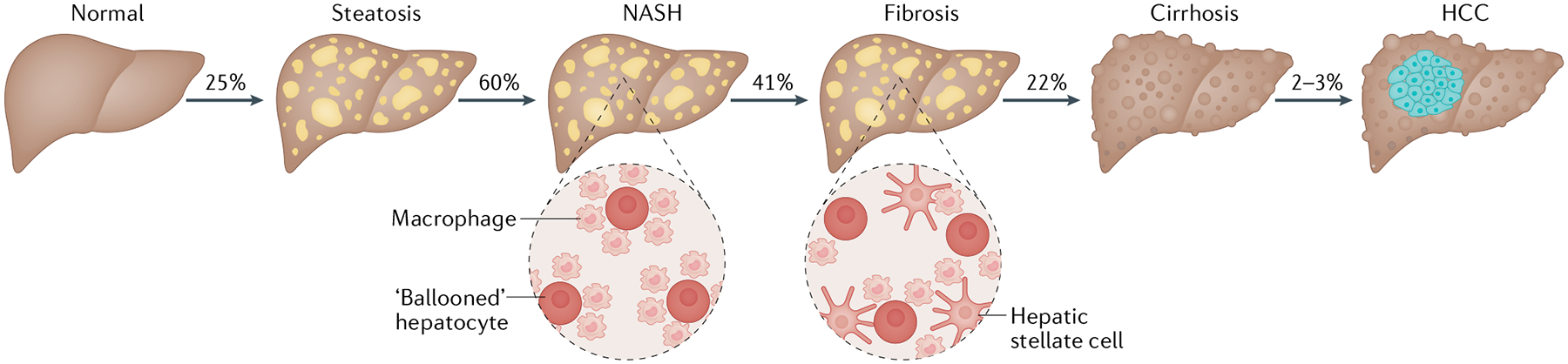
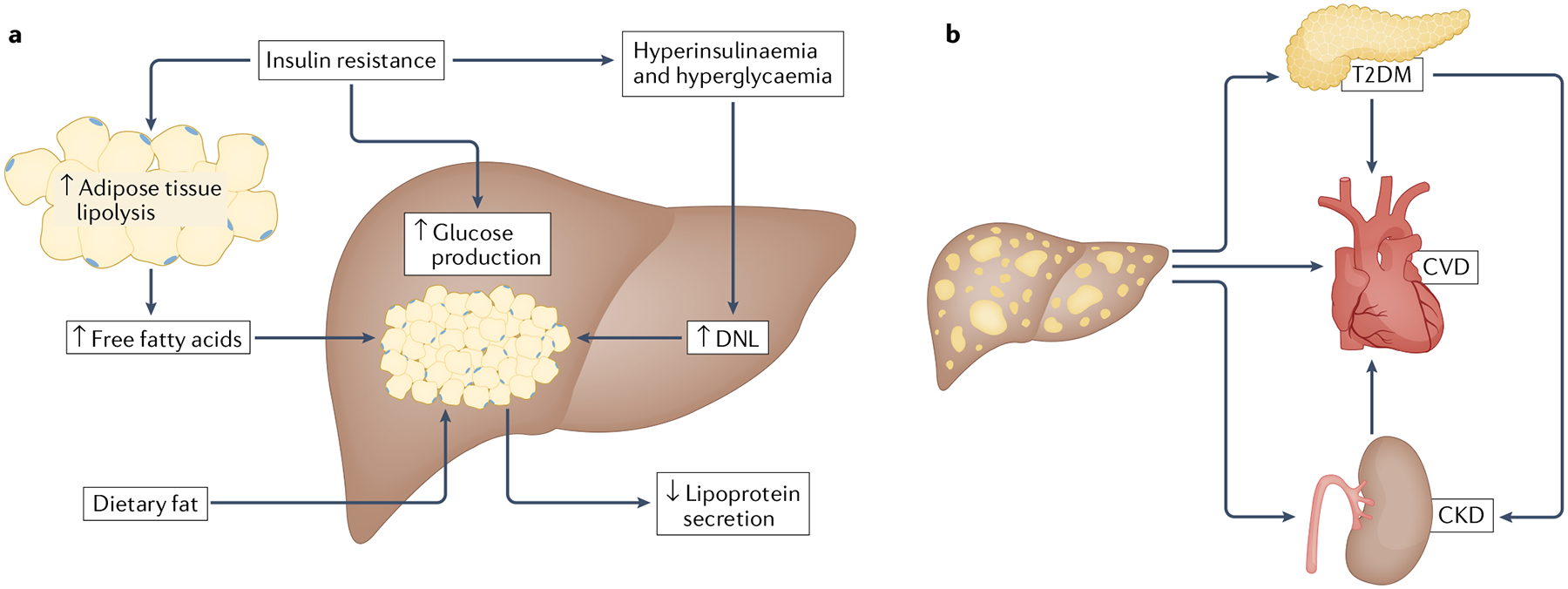
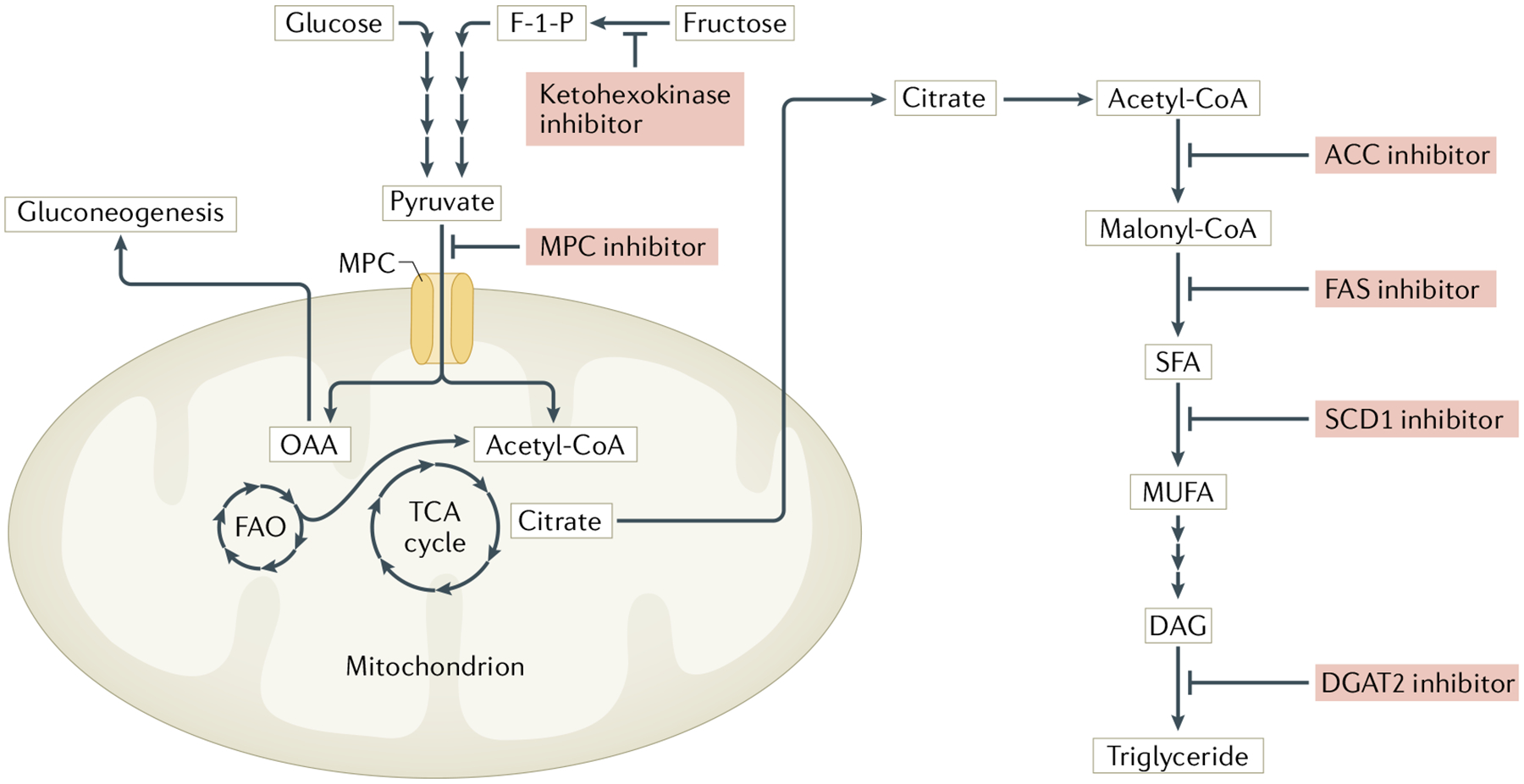
Non-alcoholic fatty liver disease (NAFLD) has emerged as the most prevalent liver disease in the world, yet there are still no approved pharmacological therapies to prevent or treat this condition. NAFLD encompasses a spectrum of severity, ranging from simple steatosis to non-alcoholic steatohepatitis (NASH). Although NASH is linked to an increased risk of hepatocellular carcinoma and cirrhosis and has now become the leading cause of liver failure-related transplantation, the majority of patients with NASH will ultimately die as a result of complications of type 2 diabetes mellitus (T2DM) and cardiometabolic diseases. Importantly, NAFLD is closely linked to obesity and tightly interrelated with insulin resistance and T2DM. Thus, targeting these interconnected conditions and taking a holistic attitude to the treatment of metabolic disease could prove to be a very beneficial approach. This Review will explore the latest relevant literature and discuss the ongoing therapeutic options for NAFLD focused on targeting intermediary metabolism, insulin resistance and T2DM to remedy the global health burden of these diseases.
© 2021. Springer Nature Limited.
Conflict of interest statement
Competing interests
B.N.F. is a stockholder and member of the scientific advisory board of Cirius Therapeutics Inc., which is developing MSDC-0602 for the treatment of NASH. D.F. declares no competing interests.
Figures
References
-
- Younossi ZM et al. Global epidemiology of nonalcoholic fatty liver disease — Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 64, 73–84 (2016). - PubMed
-
- Younossi ZM et al. The economic and clinical burden of nonalcoholic fatty liver disease in the United States and Europe. Hepatology 64, 1577–1586 (2016). - PubMed
-
- Vilar-Gomez E et al. Weight loss through lifestyle modification significantly reduces features of nonalcoholic steatohepatitis. Gastroenterology 149, 367–378 (2015). - PubMed
-
- Chalasani N et al. The diagnosis and management of nonalcoholic fatty liver disease: practice guidance from the American Association for the Study of Liver Diseases. Hepatology 67, 328–357 (2018). - PubMed
-
- Younossi ZM et al. Epidemiology of chronic liver diseases in the USA in the past three decades. Gut 69, 564–568 (2020). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
