

A rare case of paradoxical pulmonary embolism in spontaneous aortocaval fistula
- PMID: 34131500
- PMCID: PMC8171143
- DOI: 10.1259/bjrcr.20200183
A rare case of paradoxical pulmonary embolism in spontaneous aortocaval fistula
Abstract
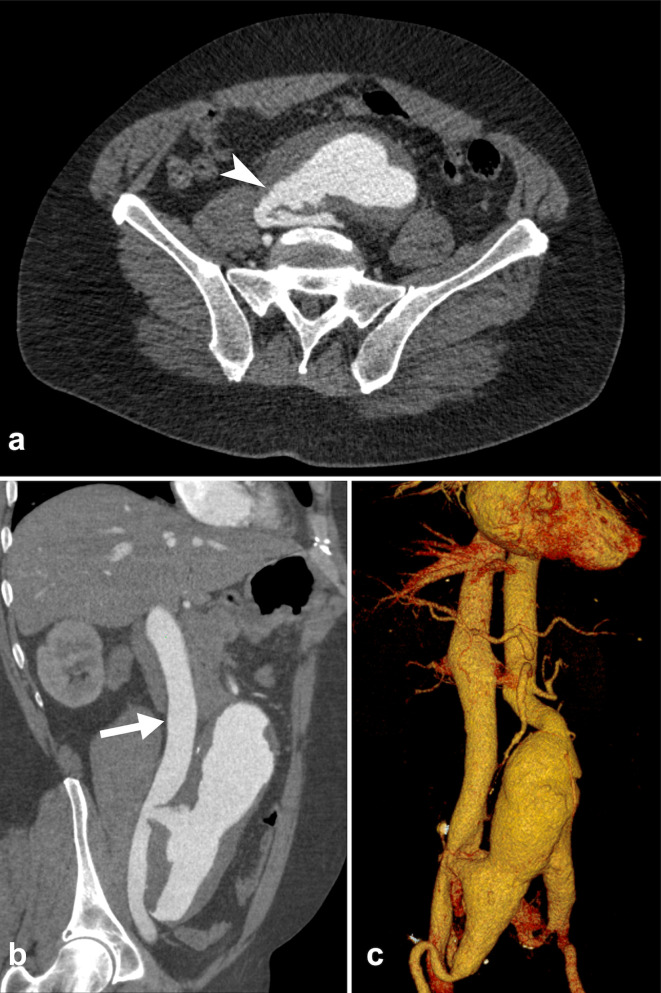
Aortocaval fistula (ACF) is a rare complication of abdominal aortic aneurysm (AAA), occurring in less than 1% of all AAAs. Paradoxical embolism can rarely be associated with ACF, pulmonary embolism may originate from dislodgment of thrombotic material from the AAA in the inferior vena cava (IVC) through the ACF. We report a case of a patient admitted to the emergency department with abdominal pain and shortness of breath who immediately underwent thoraco-abdominal CT. Imaging allowed a prompt pre-operative diagnosis of an ACF between an AAA and the IVC, also identifying CT signs of right heart overload and the presence of a paradoxical pulmonary embolism.
© 2021 The Authors. Published by the British Institute of Radiology.
Figures


References
Publication types
LinkOut - more resources
Full Text Sources
