

A rare case of accessory liver lobe torsion in a pediatric patient who showed recurrent epigastralgia and who was treated by elective laparoscopic resection
- PMID: 34131777
- PMCID: PMC8206295
- DOI: 10.1186/s40792-021-01231-6
A rare case of accessory liver lobe torsion in a pediatric patient who showed recurrent epigastralgia and who was treated by elective laparoscopic resection
Abstract
Background: Accessory liver lobe (ALL) is a rare liver malformation. An ALL develops due to malformation of the endodermal caudal foregut and segmentation of the hepatic bud in the third week of gestation. Most ALLs are asymptomatic and are detected incidentally during abdominal surgery. The incidence of ALL is < 1% in patients who undergo abdominal surgery. However, some ALLs twist and cause acute abdomen. We experienced a pediatric case of ALL torsion in a patient who underwent elective laparoscopic surgery.
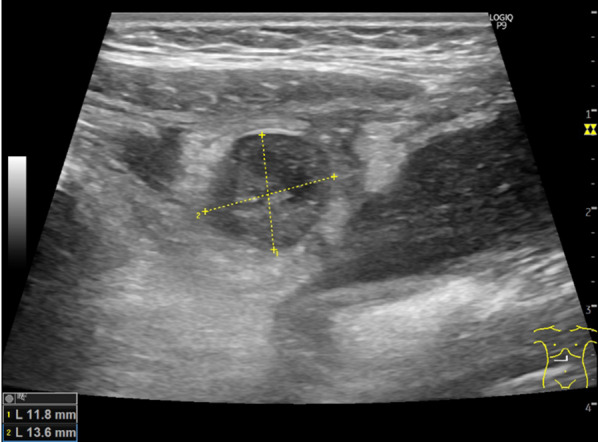
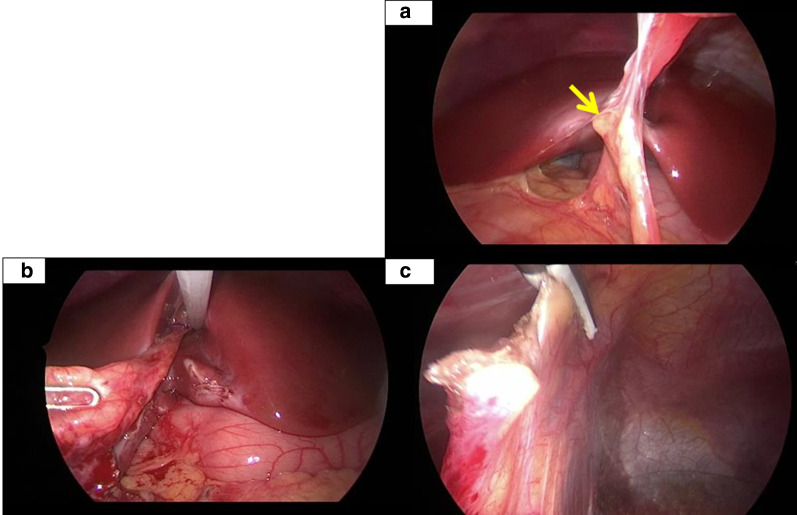
Case presentation: The 5-year-old girl had a 3-month history of epigastralgia and vomiting, which occurred every 2 weeks. Abdominal ultrasonography with color Doppler imaging revealed an 11.8 × 13.6 mm nonvascular lesion with mixed echogenicity near the round ligament of the liver. Enhanced computed tomography confirmed a 14 × 16 × 20 mm low-attenuation mass surrounded by a hyperdense line and disproportionate fat stranding on the right side of the round ligament of the liver. There was no ascites or hemorrhage. These findings suggested an abscess of the round ligament of the liver. Her symptoms improved with the administration of oral antibiotics; thus, we planned to perform elective exploratory laparoscopy and subsequent resection. Two trocars (5 mm) were inserted through a multichannel port device at the umbilicus and one trocar (3 mm) was inserted at the right lateral abdomen. Upon observation of the abdominal cavity, the omentum was observed adhering to the round ligament of the liver. Macroscopic observation revealed no apparent mass lesions. We performed adhesiolysis of the omentum from the round ligament of the liver using a vessel sealing system. We performed resection at the site at which adhesion had formed between the round ligament of the liver with the surrounding tissue using a vessel sealing system and the resected specimen was extracted through the umbilical wound. The postoperative course was uneventful. A pathological examination revealed necrotic liver tissue. The resected tissue was founded to be an ALL with ischemic change.
Conclusions: The recurrent abdominal pain was induced by torsion of the ALL. Pediatric surgeons should consider ALL torsion as a differential diagnosis for epigastralgia of unknown etiology.
Keywords: Accessory liver lobe; Children; Epigastralgia; Laparoscopic surgery; Torsion.
Conflict of interest statement
The authors declare no competing interests in association with the present study.
Figures


References
-
- Corbitt N, Rellinger EJ, Hernanz-Schulman M, Chung DH. Accessory hepatic lobes in the pediatric population; A report of three cases of torsion and literature review. J Pediatr Surg Case Rep. 2017;16:15–18. doi: 10.1016/j.epsc.2016.09.003. - DOI
LinkOut - more resources
Full Text Sources
