

A multidisciplinary approach remains the best strategy to improve and strengthen the management of ovarian cancer (Review)
- PMID: 34132354
- PMCID: PMC8208622
- DOI: 10.3892/ijo.2021.5233
A multidisciplinary approach remains the best strategy to improve and strengthen the management of ovarian cancer (Review)
Abstract
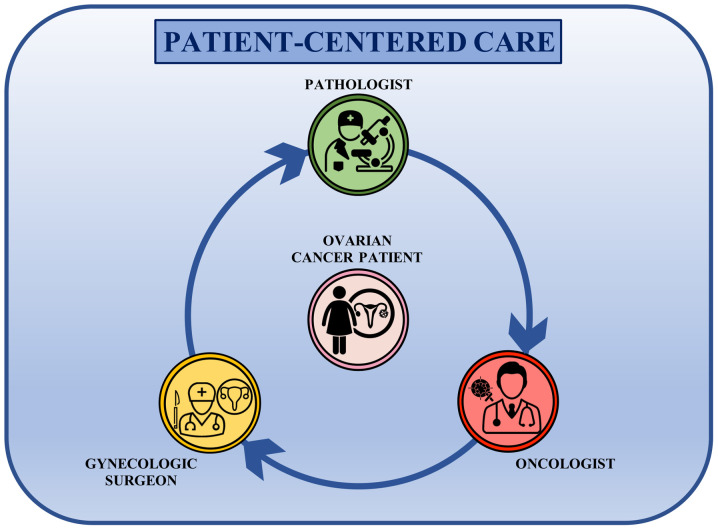
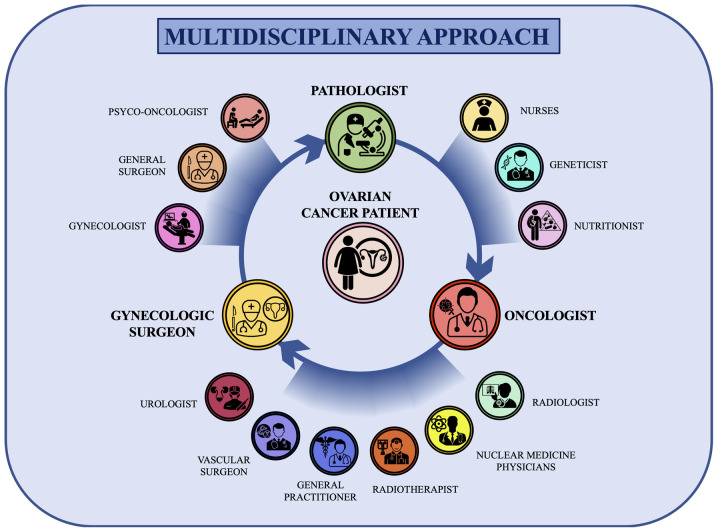
Ovarian cancer represents one of the most aggressive female tumors worldwide. Over the decades, the therapeutic options for the treatment of ovarian cancer have been improved significantly through the advancement of surgical techniques as well as the availability of novel effective drugs able to extend the life expectancy of patients. However, due to its clinical, biological and molecular complexity, ovarian cancer is still considered one of the most difficult tumors to manage. In this context, several studies have highlighted how a multidisciplinary approach to this pathology improves the prognosis and survival of patients with ovarian cancer. On these bases, the aim of the present review is to present recent advantages in the diagnosis, staging and treatment of ovarian cancer highlighting the benefits of a patient‑centered care approach and on the importance of a multidisciplinary team for the management of ovarian cancer.
Keywords: diagnosis; multidisciplinary approach; multidisciplinary team; ovarian cancer; patient‑centered care; poly (ADP‑ribose) polymerase inhibitors; staging; therapy.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical