

A Personalized Home-Based Rehabilitation Program Using Exergames Combined With a Telerehabilitation App in a Chronic Stroke Survivor: Mixed Methods Case Study
- PMID: 34132649
- PMCID: PMC8441601
- DOI: 10.2196/26153
A Personalized Home-Based Rehabilitation Program Using Exergames Combined With a Telerehabilitation App in a Chronic Stroke Survivor: Mixed Methods Case Study
Abstract
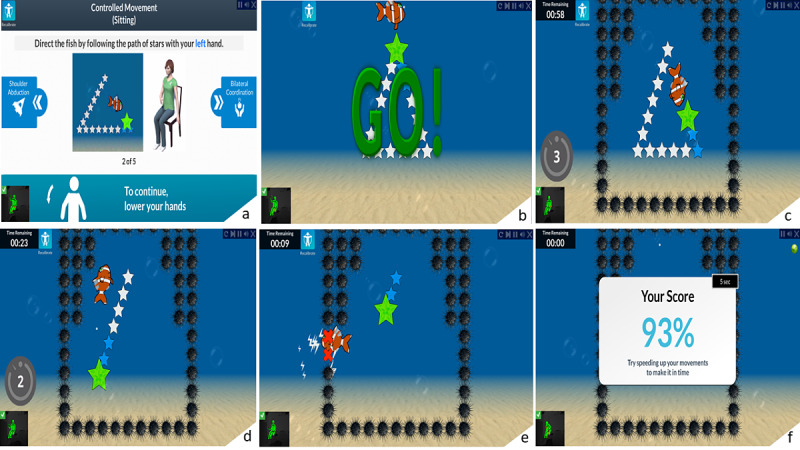
Background: In Canada, only 11% of stroke survivors have access to outpatient and community-based rehabilitation after discharge from inpatient rehabilitation. Hence, innovative community-based strategies are needed to provide adequate postrehabilitation services. The VirTele program, which combines virtual reality exergames and a telerehabilitation app, was developed to provide stroke survivors with residual upper extremity deficits, the opportunity to participate in a personalized home rehabilitation program.
Objective: This study aims to determine the feasibility of VirTele for remote upper extremity rehabilitation in a chronic stroke survivor; explore the preliminary efficacy of VirTele on upper extremity motor function, the amount and quality of upper extremity use, and impact on quality of life and motivation; and explore the determinants of behavioral intention and use behavior of VirTele along with indicators of empowerment.
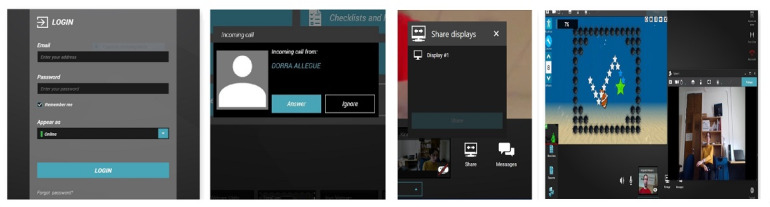
Methods: A 63-year-old male stroke survivor (3 years) with moderate upper extremity impairment participated in a 2-month VirTele intervention. He was instructed to use exergames (5 games for upper extremity) for 30 minutes, 5 times per week, and conduct videoconference sessions with a clinician at least once per week. Motivational interviewing was incorporated into VirTele to empower the participant to continue exercising and use his upper extremities in everyday activities. Upper extremity motor function (Fugl-Meyer Assessment-upper extremity), amount and quality of upper extremity use (Motor Activity Log-30), and impact on quality of life (Stroke Impact Scale-16) and motivation (Treatment Self-Regulation Questionnaire-15) were measured before (T1), after (T2) VirTele intervention, and during a 1- (T3) and 2-month (T4) follow-up period. Qualitative data were collected through logs and semistructured interviews. Feasibility data (eg, number and duration of videoconference sessions and adherence) were documented at the end of each week.
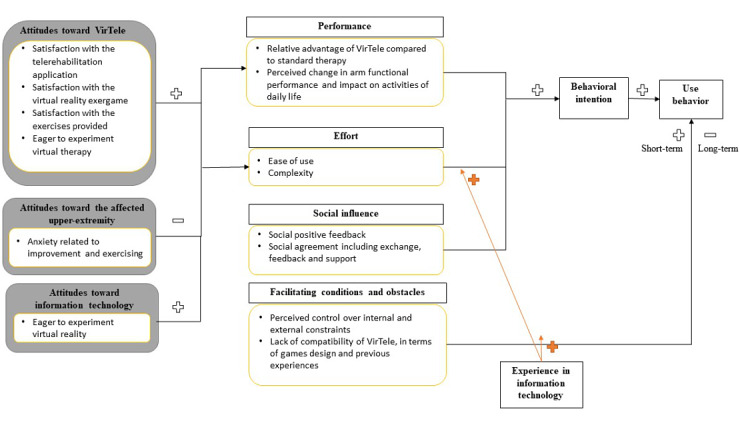
Results: The participant completed 48 exergame sessions (33 hours) and 8 videoconference sessions. Results suggest that the VirTele intervention and the study protocol could be feasible for stroke survivors. The participant exhibited clinically meaningful improvements at T2 on the Fugl-Meyer and Stroke Impact Scale-16 and maintained these gains at T3 and T4. During the follow-up periods, the amount and quality of upper extremity use showed meaningful changes, suggesting more involvement of the affected upper extremity in daily activities. The participant demonstrated a high level of autonomous motivation, which may explain his adherence. Performance, effort, and social influence have meaningful weights in the behavioral intention of using VirTele. However, the lack of control of technical and organizational infrastructures may influence the long-term use of technology. At the end of the intervention, the participant demonstrated considerable empowerment at both the behavioral and capacity levels.
Conclusions: VirTele was shown to be feasible for use in chronic stroke survivors for remote upper extremity rehabilitation. Meaningful determinants of behavioral intention and use behavior of VirTele were identified, and preliminary efficacy results are promising.
International registered report identifier (irrid): RR2-10.2196/14629.
Keywords: motivation; rehabilitation; stroke; telerehabilitation; upper extremity; video games; virtual reality.
©Dorra Rakia Allegue, Dahlia Kairy, Johanne Higgins, Philippe S Archambault, Francois Michaud, William C Miller, Shane N Sweet, Michel Tousignant. Originally published in JMIR Serious Games (https://games.jmir.org), 31.08.2021.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
Rehabilitation of Upper Extremity by Telerehabilitation Combined With Exergames in Survivors of Chronic Stroke: Preliminary Findings From a Feasibility Clinical Trial.JMIR Rehabil Assist Technol. 2022 Jun 22;9(2):e33745. doi: 10.2196/33745. JMIR Rehabil Assist Technol. 2022. PMID: 35731560 Free PMC article.
-
Lessons Learned From Clinicians and Stroke Survivors About Using Telerehabilitation Combined With Exergames: Multiple Case Study.JMIR Rehabil Assist Technol. 2022 Sep 15;9(3):e31305. doi: 10.2196/31305. JMIR Rehabil Assist Technol. 2022. PMID: 36107484 Free PMC article.
-
Optimization of Upper Extremity Rehabilitation by Combining Telerehabilitation With an Exergame in People With Chronic Stroke: Protocol for a Mixed Methods Study.JMIR Res Protoc. 2020 May 21;9(5):e14629. doi: 10.2196/14629. JMIR Res Protoc. 2020. PMID: 32097119 Free PMC article.
-
Comparing Ways to Treat Arm Weakness Due to Stroke [Internet].Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2021 May. Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2021 May. PMID: 38556969 Free Books & Documents. Review.
-
Effectiveness of Virtual Reality- and Gaming-Based Interventions for Upper Extremity Rehabilitation Poststroke: A Meta-analysis.Arch Phys Med Rehabil. 2020 May;101(5):885-896. doi: 10.1016/j.apmr.2019.10.195. Epub 2019 Dec 7. Arch Phys Med Rehabil. 2020. PMID: 31821799
Cited by
-
Rehabilitation of Upper Extremity by Telerehabilitation Combined With Exergames in Survivors of Chronic Stroke: Preliminary Findings From a Feasibility Clinical Trial.JMIR Rehabil Assist Technol. 2022 Jun 22;9(2):e33745. doi: 10.2196/33745. JMIR Rehabil Assist Technol. 2022. PMID: 35731560 Free PMC article.
-
Telerehabilitation for upper limb disabilities: a scoping review on functions, outcomes, and evaluation methods.Arch Public Health. 2022 Aug 23;80(1):196. doi: 10.1186/s13690-022-00952-w. Arch Public Health. 2022. PMID: 35999548 Free PMC article.
-
Stroke patients' knowledge, attitudes, and practices regarding home-based exercise and psychological rehabilitation programs.Front Med (Lausanne). 2025 Jun 26;12:1598489. doi: 10.3389/fmed.2025.1598489. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40641977 Free PMC article.
-
Behavior Change Approaches in Digital Technology-Based Physical Rehabilitation Interventions Following Stroke: Scoping Review.J Med Internet Res. 2024 Apr 24;26:e48725. doi: 10.2196/48725. J Med Internet Res. 2024. PMID: 38656777 Free PMC article.
-
Lessons Learned From Clinicians and Stroke Survivors About Using Telerehabilitation Combined With Exergames: Multiple Case Study.JMIR Rehabil Assist Technol. 2022 Sep 15;9(3):e31305. doi: 10.2196/31305. JMIR Rehabil Assist Technol. 2022. PMID: 36107484 Free PMC article.
References
-
- 2009 Tracking Heart Disease and Stroke in Canada. Ottawa: Public Health Agency of Canada; 2009.
-
- Life After Strokes. 2014. [2020-10-26]. http://canadianstrokenetwork.ca/fr/service/bulletin-sur-lavc-2014/
-
- Hebert D, Lindsay MP, McIntyre A, Kirton A, Rumney PG, Bagg S, Bayley M, Dowlatshahi D, Dukelow S, Garnhum M, Glasser E, Halabi M, Kang E, MacKay-Lyons M, Martino R, Rochette A, Rowe S, Salbach N, Semenko B, Stack B, Swinton L, Weber V, Mayer M, Verrilli S, DeVeber G, Andersen J, Barlow K, Cassidy C, Dilenge M, Fehlings D, Hung R, Iruthayarajah J, Lenz L, Majnemer A, Purtzki J, Rafay M, Sonnenberg LK, Townley A, Janzen S, Foley N, Teasell R. Canadian stroke best practice recommendations: stroke rehabilitation practice guidelines, update 2015. Int J Stroke. 2016 Jun;11(4):459–84. doi: 10.1177/1747493016643553.1747493016643553 - DOI - PubMed
-
- Weiss P, Keshner E, Levin M. Virtual Reality for Physical and Motor Rehabilitation. Berlin, Germany: Springer; 2014.
LinkOut - more resources
Full Text Sources
Miscellaneous
