

Early Prehospital Tranexamic Acid Following Injury Is Associated With a 30-day Survival Benefit: A Secondary Analysis of a Randomized Clinical Trial
- PMID: 34132695
- PMCID: PMC8480233
- DOI: 10.1097/SLA.0000000000005002
Early Prehospital Tranexamic Acid Following Injury Is Associated With a 30-day Survival Benefit: A Secondary Analysis of a Randomized Clinical Trial
Abstract
Objective: We sought to characterize the timing of administration of prehospital tranexamic acid (TXA) and associated outcome benefits.
Background: TXA has been shown to be safe in the prehospital setting post-injury.
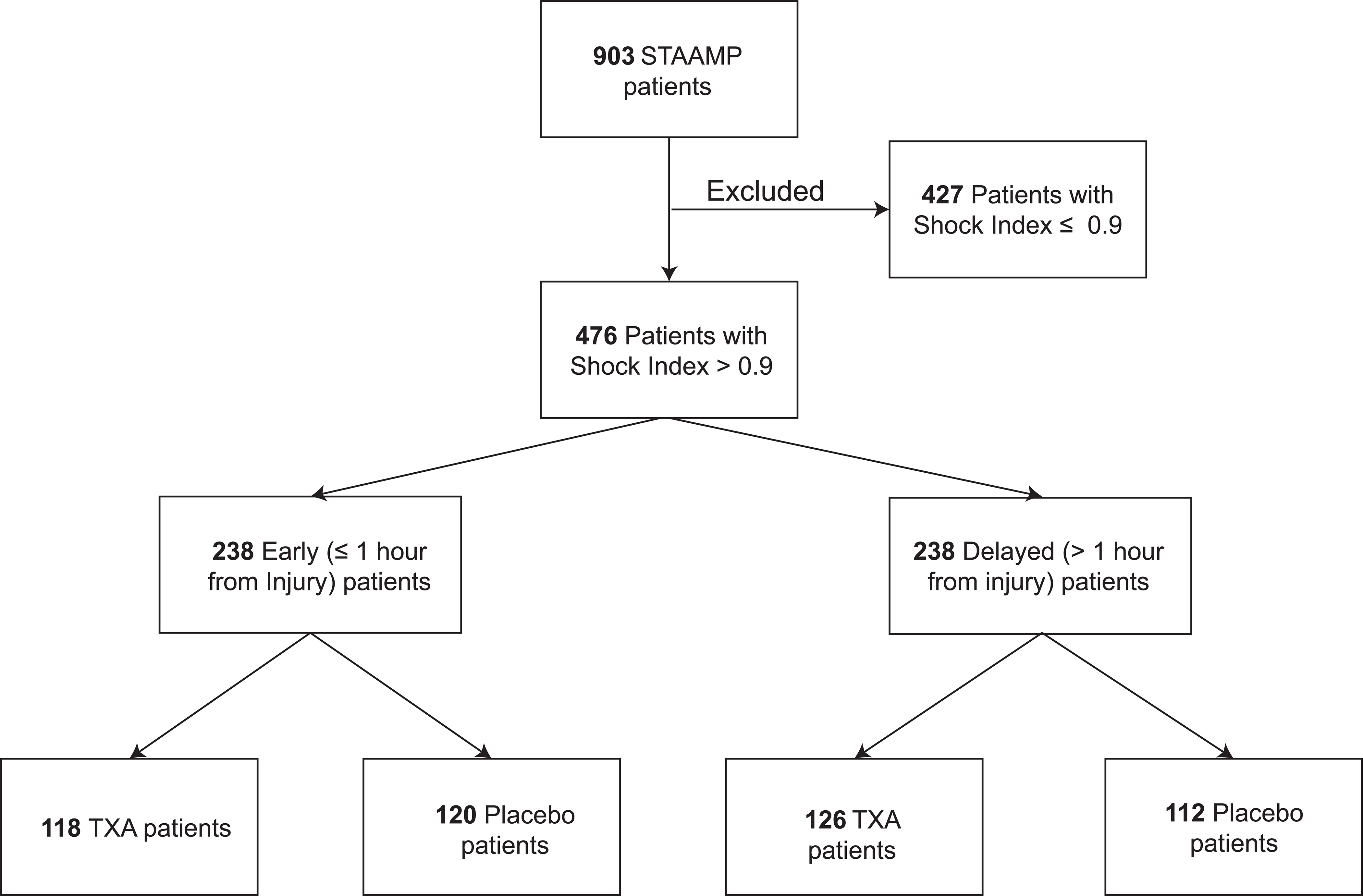
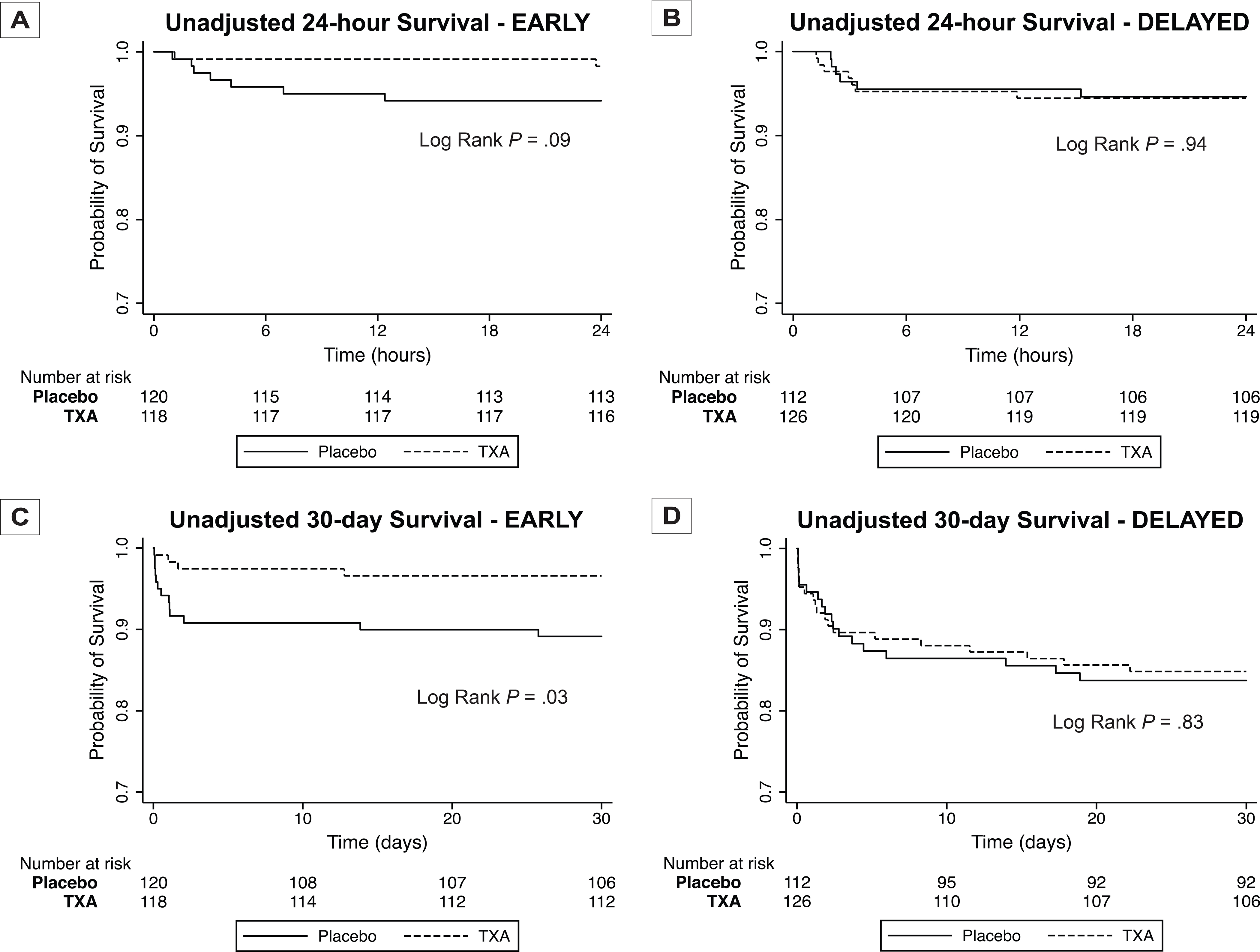
Methods: We performed a secondary analysis of a recent prehospital randomized TXA clinical trial in injured patients. Those who received prehospital TXA within 1 hour (EARLY) from time of injury were compared to those who received prehospital TXA beyond 1 hour (DELAYED). We included patients with a shock index of >0.9. Primary outcome was 30-day mortality. Kaplan-Meier and Cox Hazard regression were utilized to characterize mortality relationships.
Results: EARLY and DELAYED patients had similar demographics, injury characteristics, and shock severity but DELAYED patients had greater prehospital resuscitation requirements and longer prehospital times. Stratified Kaplan-Meier analysis demonstrated significant separation for EARLY patients (N = 238, log-rank chi-square test, 4.99; P = 0.03) with no separation for DELAYED patients (N = 238, log-rank chi-square test, 0.04; P = 0.83). Stratified Cox Hazard regression verified, after controlling for confounders, that EARLY TXA was associated with a 65% lower independent hazard for 30-day mortality [hazard ratio (HR) 0.35, 95% confidence interval (CI) 0.19-0.65, P = 0.001] with no independent survival benefit found in DELAYED patients (HR 1.00, 95% CI 0.63-1.60, P = 0.999). EARLY TXA patients had lower incidence of multiple organ failure and 6-hour and 24-hour transfusion requirements compared to placebo.
Conclusions: Administration of prehospital TXA within 1 hour from injury in patients at risk of hemorrhage is associated with 30-day survival benefit, lower incidence of multiple organ failure, and lower transfusion requirements.
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Kauvar DS, Lefering R, Wade CE. Impact of hemorrhage on trauma outcome: an overview of epidemiology, clinical presentations, and therapeutic considerations. J Trauma 2006; 60(6 Suppl):S3–11. - PubMed
-
- MacLeod JB, Lynn M, McKenney MG, et al.Early coagulopathy predicts mortality in trauma. J Trauma 2003; 55(1):39–44. - PubMed
-
- Niles SE, McLaughlin DF, Perkins JG, et al.Increased mortality associated with the early coagulopathy of trauma in combat casualties. J Trauma 2008; 64(6):1459–1463; discussion 1463–1465. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
