

Use of Lipid-Lowering Therapies Over 2 Years in GOULD, a Registry of Patients With Atherosclerotic Cardiovascular Disease in the US
- PMID: 34132735
- PMCID: PMC8209562
- DOI: 10.1001/jamacardio.2021.1810
Use of Lipid-Lowering Therapies Over 2 Years in GOULD, a Registry of Patients With Atherosclerotic Cardiovascular Disease in the US
Abstract
Importance: Guidelines for patients with atherosclerotic cardiovascular disease (ASCVD) recommend intensive statin therapy and adding nonstatin therapy if low-density lipoprotein cholesterol (LDL-C) levels are 70 mg/dL or more. Compliance with guidelines is often low.
Objective: To track LDL-C treatment patterns in the US over 2 years.
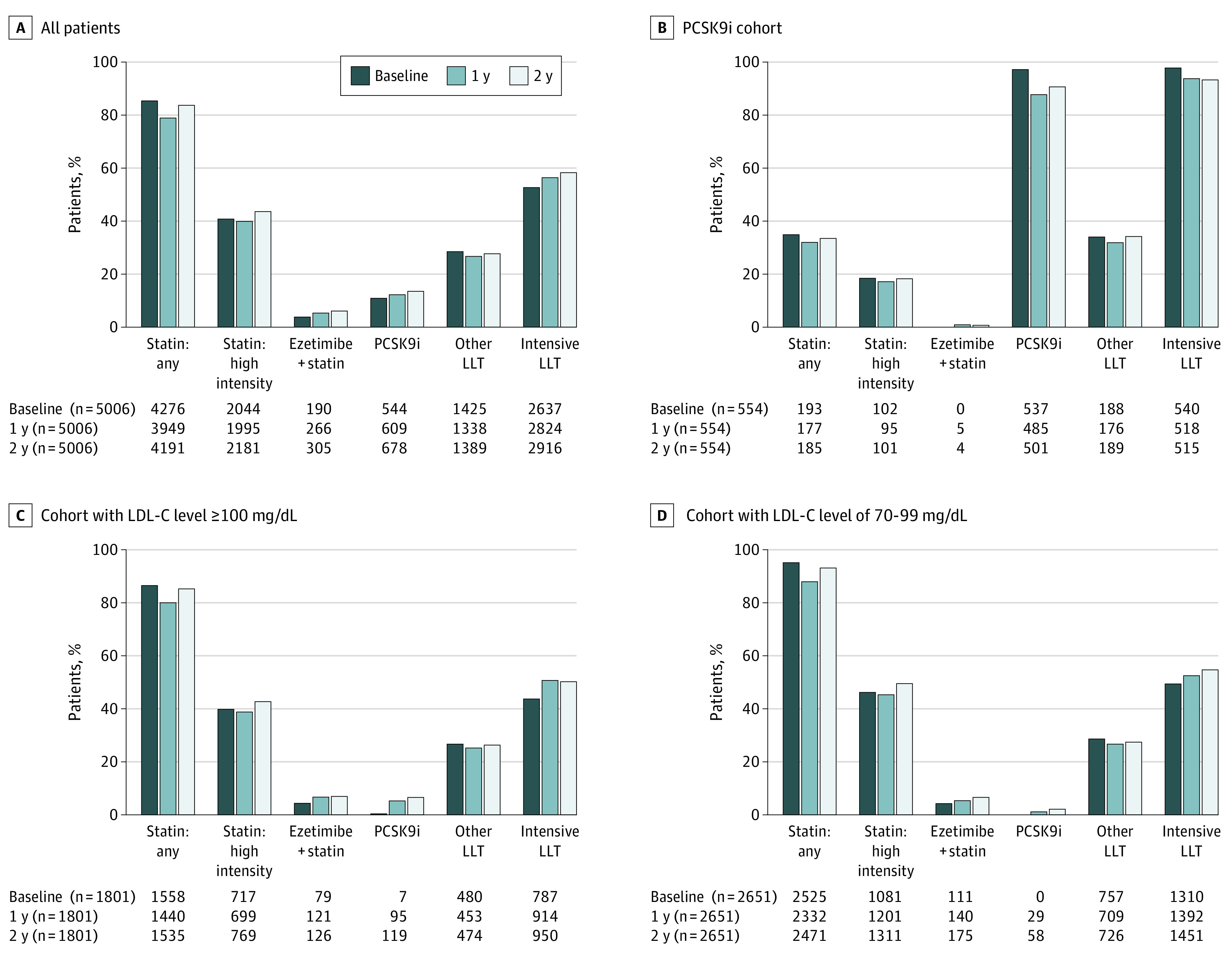
Design, setting, and participants: GOULD is a prospective observational registry study involving multiple centers. Patients with ASCVD receiving any lipid-lowering therapy (LLT) were eligible. Between December 2016 and July 2018, patients were enrolled in 1 of 3 cohorts: (1) those currently receiving proprotein convertase subtilisin/kexin type 9 inhibitor (PCSK9i) and 2 groups not receiving PCSK9i drugs, with (2) LDL-C levels of 100 mg/dL or more or (3) LDL-C levels of 70 to 99 mg/dL. Patients had medical record reviews and telephone interviews every 6 months. Analysis was done on data collected as of October 5, 2020.
Main outcomes and measures: The primary outcome was the change in LLT use in 2 years. Secondary outcomes included the number of LDL-C measurements, LDL-C levels, and responses to structured physician and patient questionnaires over 2 years.
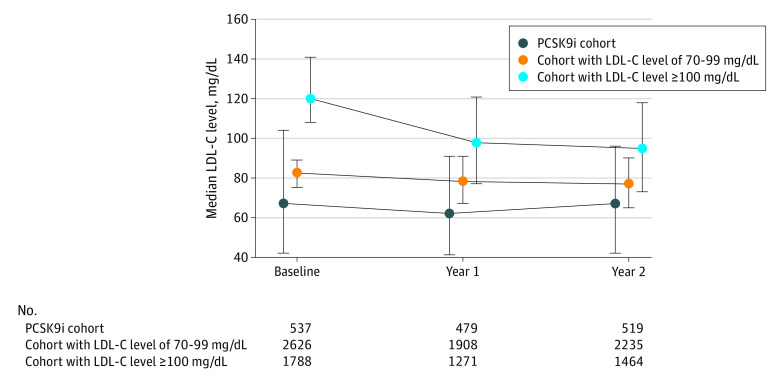
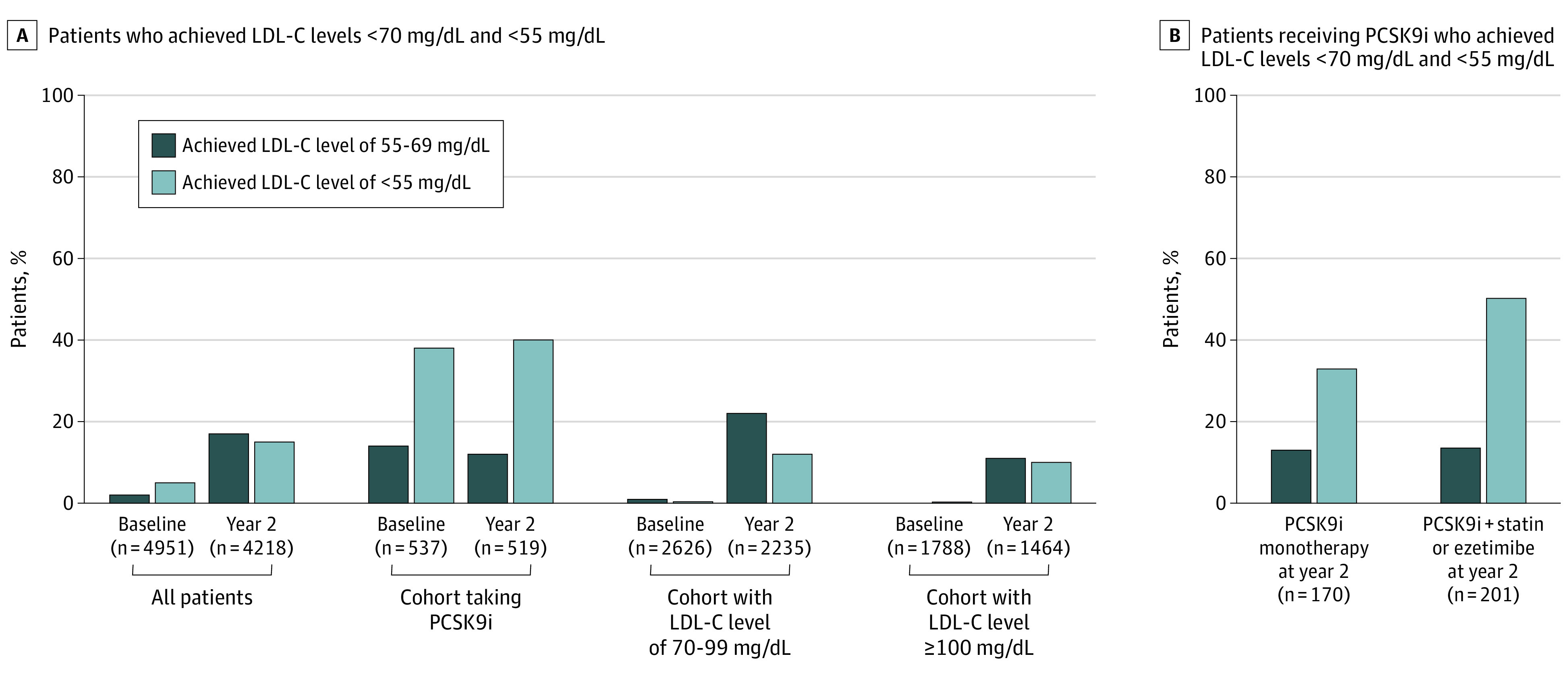
Results: A total of 5006 patients were enrolled (mean [SD] age, 67.8 [9.9] years; 1985 women [39.7%]; 4312 White individuals [86.1%]). At 2 years, 885 (17.1%) had LLT intensification. In the cohorts with LDL-C levels of 100 mg/dL or more and 70 to 99 mg/dL, LLT intensification occurred in 403 (22.4%) and 383 (14.4%), respectively; statins were intensified in 115 (6.4%) and 168 (6.3%), ezetimibe added in 123 (6.8%) and 118 (4.5%), and PCSK9i added in 114 (6.3%) and 58 (2.2%), respectively. In the PCSK9i cohort, 508 of 554 (91.7%) were still taking PCSK9i at 2 years. Lipid panels were measured at least once over 2 years in 3768 patients (88.5%; PCSK9i cohort, 492 [96.1%]; LDL-C levels ≥100 mg/dL or more, 1294 [85.9%]; 70-99 mg/dL, 1982 [88.6%]). Levels of LDL-C fell from medians (interquartile ranges) of 120 (108-141) mg/dL to 95 (73-118) mg/dL in the cohort with LDL-C levels of 100 mg/dL or more, 82 (75-89) to 77 (65-90) mg/dL in the cohort with LDL-C levels of 70 to 99 mg/dL, and 67 (42-104) mg/dL to 67 (42-96) mg/dL in the PCSK9i cohort. Levels of LDL-C less than 70 mg/dL at 2 years were achieved by 308 patients (21.0%) and 758 patients (33.9%) in the cohorts with LDL-C levels of 100 mg/dL or more and 70 to 99 mg/dL, respectively, and 272 patients (52.4%) in the PCSK9i cohort. At 2 years, practice characteristics were associated with more LLT intensification (teaching vs nonteaching hospitals, 148 of 589 [25.1%] vs 600 of 3607 [16.6%]; lipid protocols or none, 359 of 1612 [22.3%] vs 389 of 2584 [15.1%]; cardiology, 452 of 2087 [21.7%] vs internal or family medicine, 204 of 1745 [11.7%] and other, 92 of 364 [25.3%]; all P < .001) and achievement of LDL-C less than 70 mg/dL (teaching vs nonteaching hospitals, 173 of 488 [35.5%] vs 823 of 2986 [27.6%]; lipid protocols vs none, 451 of 1411 [32.0%] vs 545 of 2063 [26.4%]; both P < .001; cardiology, 523 of 1686 [30.1%] vs internal or family medicine, 377 of 1472 [25.6%] and other, 96 of 316 [30.4%]; P = .003).
Conclusions and relevance: Of patients with ASCVD, most with suboptimal LDL-C levels at baseline, only 17.1% had LLT intensification after 2 years, and two-thirds remained at an LDL-C level greater than 70 mg/dL. Further intensive efforts are needed to achieve optimal LDL-C management in patients with ASCVD.
Conflict of interest statement
Figures
References
-
- Baigent C, Blackwell L, Emberson J, et al. ; Cholesterol Treatment Trialists’ (CTT) Collaboration . Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376(9753):1670-1681. doi:10.1016/S0140-6736(10)61350-5 - DOI - PMC - PubMed
-
- Cannon CP, Braunwald E, McCabe CH, et al. ; Pravastatin or Atorvastatin Evaluation and Infection Therapy-Thrombolysis in Myocardial Infarction 22 Investigators . Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med. 2004;350(15):1495-1504. doi:10.1056/NEJMoa040583 - DOI - PubMed
