

Neurocognitive Functioning in Individuals at Clinical High Risk for Psychosis: A Systematic Review and Meta-analysis
- PMID: 34132736
- PMCID: PMC8209603
- DOI: 10.1001/jamapsychiatry.2021.1290
Neurocognitive Functioning in Individuals at Clinical High Risk for Psychosis: A Systematic Review and Meta-analysis
Abstract
Importance: Neurocognitive functioning is a potential biomarker to advance detection, prognosis, and preventive care for individuals at clinical high risk for psychosis (CHR-P). The current consistency and magnitude of neurocognitive functioning in individuals at CHR-P are undetermined.
Objective: To provide an updated synthesis of evidence on the consistency and magnitude of neurocognitive functioning in individuals at CHR-P.
Data sources: Web of Science database, Cochrane Central Register of Reviews, and Ovid/PsycINFO and trial registries up to July 1, 2020.
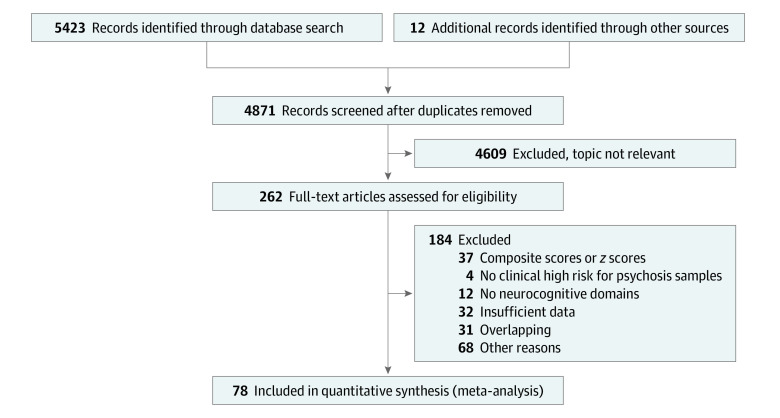
Study selection: Multistep literature search compliant with Preferred Reporting Items for Systematic Reviews and Meta-analyses and Meta-analysis of Observational Studies in Epidemiology performed by independent researchers to identify original studies reporting on neurocognitive functioning in individuals at CHR-P.
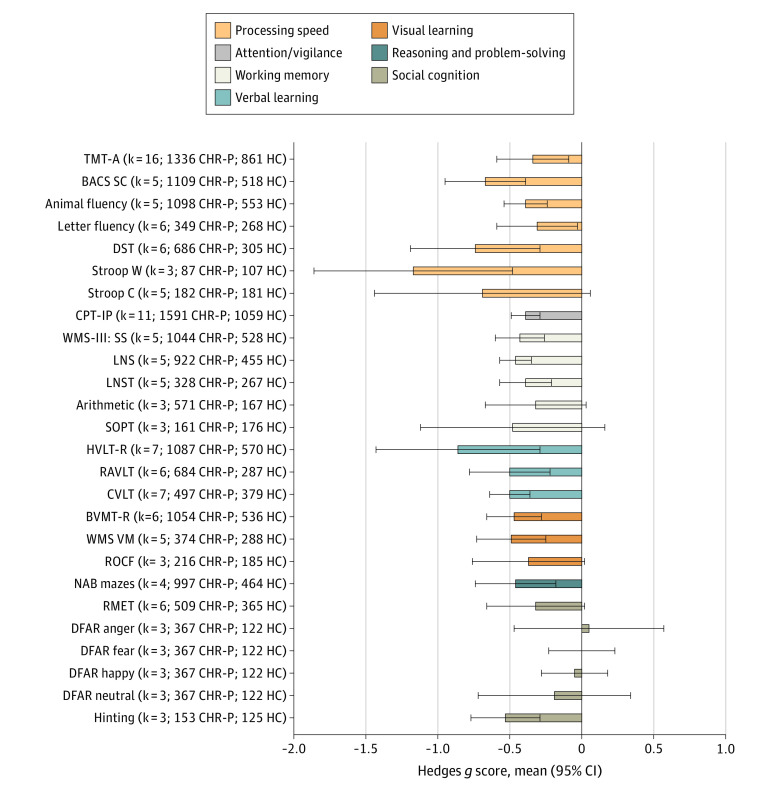
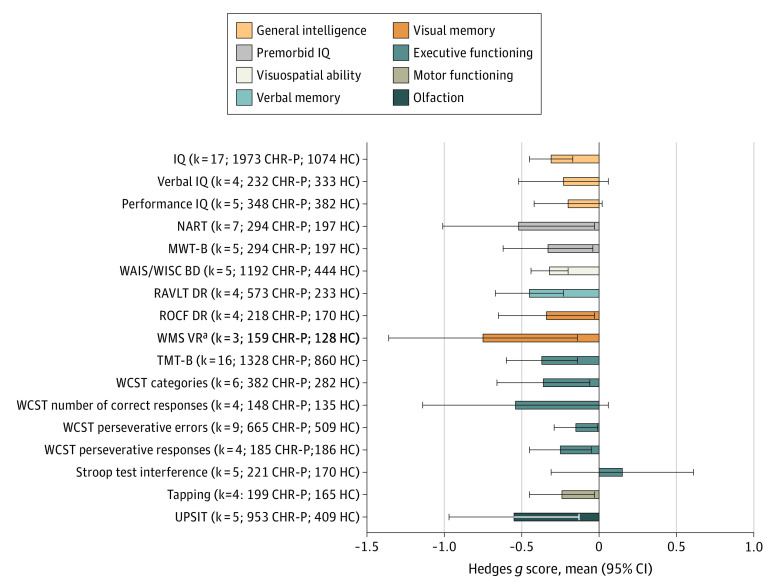
Data extraction and synthesis: Independent researchers extracted the data, clustering the neurocognitive tasks according to 7 Measurement and Treatment Research to Improve Cognition in Schizophrenia (MATRICS) domains and 8 CHR-P domains. Random-effect model meta-analyses, assessment of publication biases and study quality, and meta-regressions were conducted.
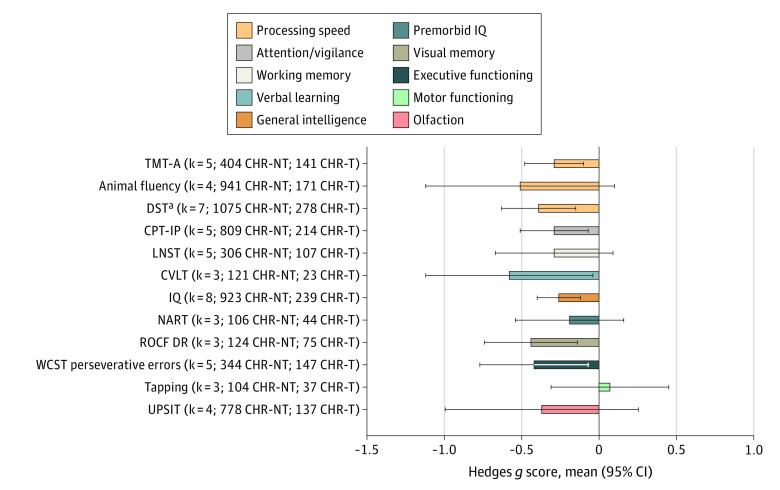
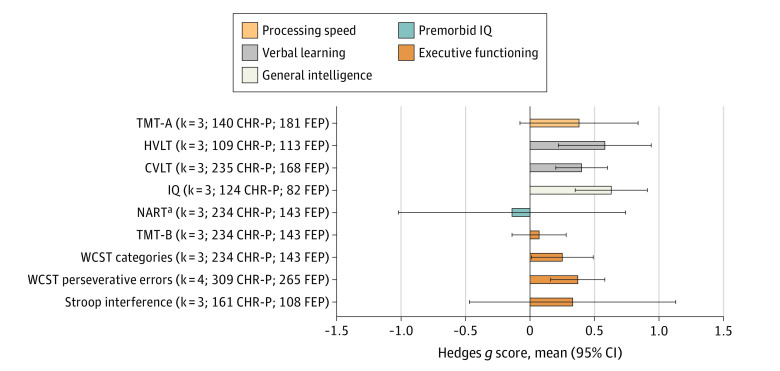
Main outcomes and measures: The primary effect size measure was Hedges g of neurocognitive functioning in individuals at CHR-P (1) compared with healthy control (HC) individuals or (2) compared with individuals with first-episode psychosis (FEP) or (3) stratified for the longitudinal transition to psychosis.
Results: A total of 78 independent studies were included, consisting of 5162 individuals at CHR-P (mean [SD; range] age, 20.2 [3.3; 12.0-29.0] years; 2529 [49.0%] were female), 2865 HC individuals (mean [SD; range] age, 21.1 [3.6; 12.6-29.2] years; 1490 [52.0%] were female), and 486 individuals with FEP (mean [SD; range] age, 23.0 [2.0; 19.1-26.4] years; 267 [55.9%] were female). Compared with HC individuals, individuals at CHR-P showed medium to large deficits on the Stroop color word reading task (g = -1.17; 95% CI, -1.86 to -0.48), Hopkins Verbal Learning Test-Revised (g = -0.86; 95% CI, -1.43 to -0.28), digit symbol coding test (g = -0.74; 95% CI, -1.19 to -0.29), Brief Assessment of Cognition Scale Symbol Coding (g = -0.67; 95% CI, -0.95 to -0.39), University of Pennsylvania Smell Identification Test (g = -0.55; 95% CI, -0.97 to -0.12), Hinting Task (g = -0.53; 95% CI, -0.77 to -0.28), Rey Auditory Verbal Learning Test (g = -0.50; 95% CI, -0.78 to -0.21), California Verbal Learning Test (CVLT) (g = -0.50; 95% CI, -0.64 to -0.36), and National Adult Reading Test (g = -0.52; 95% CI, -1.01 to -0.03). Individuals at CHR-P were less impaired than individuals with FEP. Longitudinal transition to psychosis from a CHR-P state was associated with medium to large deficits in the CVLT task (g = -0.58; 95% CI, -1.12 to -0.05). Meta-regressions found significant effects for age and education on processing speed.
Conclusions and relevance: Findings from this meta-analysis support neurocognitive dysfunction as a potential detection and prognostic biomarker in individuals at CHR-P. These findings may advance clinical research and inform preventive approaches.
Conflict of interest statement
Figures
Comment in
References
-
- National Institute for Health and Care Excellence NICE Guideline . Psychosis and schizophrenia in adults: prevention and management. Accessed December 1, 2020. https://www.nice.org.uk/guidance/cg178
LinkOut - more resources
Full Text Sources
Other Literature Sources
