

Association of Demographic Factors and Infantile Hemangioma Characteristics With Risk of PHACE Syndrome
- PMID: 34132754
- PMCID: PMC8209569
- DOI: 10.1001/jamadermatol.2021.1901
Association of Demographic Factors and Infantile Hemangioma Characteristics With Risk of PHACE Syndrome
Erratum in
-
Incorrect Author Name.JAMA Dermatol. 2021 Aug 1;157(8):1008. doi: 10.1001/jamadermatol.2021.2991. JAMA Dermatol. 2021. PMID: 34406345 Free PMC article. No abstract available.
Abstract
Importance: A 2010 prospective study of 108 infants estimated the incidence of PHACE (posterior fossa malformations, hemangioma, arterial anomalies, cardiac defects, eye anomalies) syndrome to be 31% in children with facial infantile hemangiomas (IHs) of at least 22 cm2. There is little evidence regarding the associations among IH characteristics, demographic characteristics, and risk of PHACE syndrome.
Objectives: To evaluate demographic characteristics and comorbidities in a large cohort of patients at risk for PHACE syndrome and assess the clinical features of large head and neck IH that may be associated with a greater risk of a diagnosis of PHACE syndrome.
Design, setting, and participants: This multicenter, retrospective cohort study assessed all patients with a facial, head, and/or neck IH who were evaluated for PHACE syndrome from August 1, 2009, to December 31, 2014, at 13 pediatric dermatology referral centers across North America. Data analysis was performed from June 15, 2017, to February 29, 2020.
Main outcomes and measures: The main outcome was presence or absence of PHACE syndrome. Data included age at diagnosis, sex, patterns of IH presentation (including size, segment location, and depth), diagnostic procedures and results, and type and number of associated anomalies.
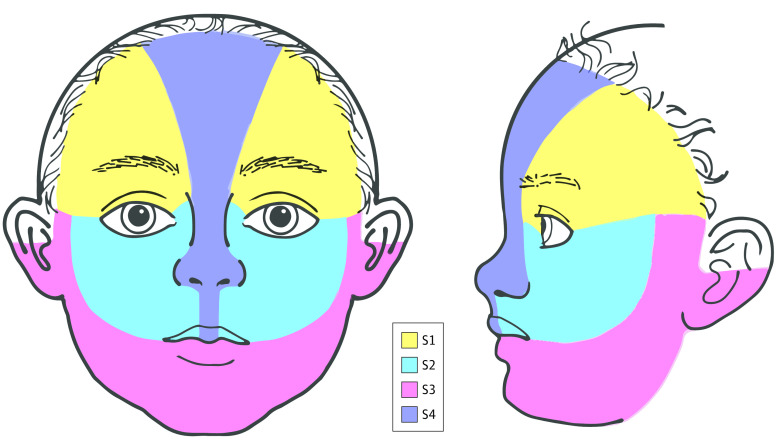
Results: A total of 238 patients (mean [SD] age, 2.96 [4.71] months; 184 [77.3%] female) were included in the analysis; 106 (44.5%) met the criteria for definite (n = 98) or possible (n = 8) PHACE syndrome. A stepwise linear regression model found that a surface area of 25 cm2 or greater (odds ratio [OR] 2.99; 95% CI, 1.49-6.02) and involvement of 3 or more locations (OR, 17.96; 95% CI, 6.10-52.85) to be statistically significant risk factors for PHACE syndrome. Involvement of the parotid gland (OR, 0.39; 95% CI, 0.18-0.85) and segment S2 (OR, 0.38; 95% CI, 0.16-0.91) was associated with a lower risk. Race and ethnicity may also be associated with PHACE syndrome risk, although more studies are needed.
Conclusions and relevance: This cohort study further described factors associated with both a higher and lower risk of PHACE syndrome. The presence of multiple anatomical sites and large surface area were associated with greater risk, whereas S2 or parotid IHs were associated with lower, but still potential, risk. These findings can help in counseling families and decision-making regarding evaluation of infants with large head and neck IHs.
Conflict of interest statement
Figures

References
LinkOut - more resources
Full Text Sources
Miscellaneous
