

COVID-19-related mortality in kidney transplant and haemodialysis patients: a comparative, prospective registry-based study
- PMID: 34132811
- PMCID: PMC8394823
- DOI: 10.1093/ndt/gfab200
COVID-19-related mortality in kidney transplant and haemodialysis patients: a comparative, prospective registry-based study
Abstract
Background: Coronavirus disease 2019 (COVID-19) has exposed haemodialysis (HD) patients and kidney transplant (KT) recipients to an unprecedented life-threatening infectious disease, raising concerns about kidney replacement therapy (KRT) strategy during the pandemic. This study investigated the association of the type of KRT with COVID-19 severity, adjusting for differences in individual characteristics.
Methods: Data on KT recipients and HD patients diagnosed with COVID-19 between 1 February 2020 and 1 December 2020 were retrieved from the European Renal Association COVID-19 Database. Cox regression models adjusted for age, sex, frailty and comorbidities were used to estimate hazard ratios (HRs) for 28-day mortality risk in all patients and in the subsets that were tested because of symptoms.
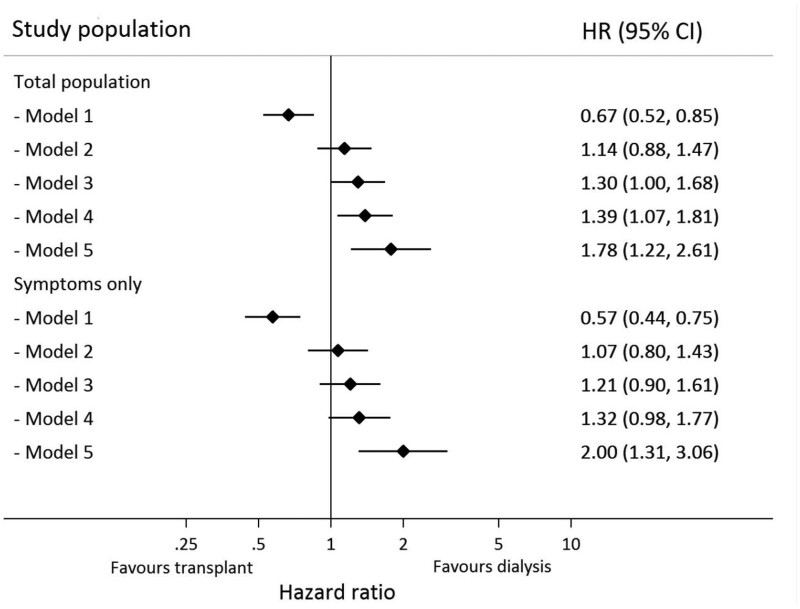
Results: A total of 1670 patients (496 functional KT and 1174 HD) were included; 16.9% of KT and 23.9% of HD patients died within 28 days of presentation. The unadjusted 28-day mortality risk was 33% lower in KT recipients compared with HD patients {HR 0.67 [95% confidence interval (CI) 0.52-0.85]}. In a fully adjusted model, the risk was 78% higher in KT recipients [HR 1.78 (95% CI 1.22-2.61)] compared with HD patients. This association was similar in patients tested because of symptoms [fully adjusted model HR 2.00 (95% CI 1.31-3.06)]. This risk was dramatically increased during the first post-transplant year. Results were similar for other endpoints (e.g. hospitalization, intensive care unit admission and mortality >28 days) and across subgroups.
Conclusions: KT recipients had a greater risk of a more severe course of COVID-19 compared with HD patients, therefore they require specific infection mitigation strategies.
Keywords: COVID-19; dialysis; kidney; mortality; transplantation.
© The Author(s) 2021. Published by Oxford University Press on behalf of ERA-EDTA.
Figures
References
-
- European Centre for Disease Prevention and Control. COVID-19 situation update for the EU/EEA. https://www.ecdc.europa.eu/en/cases-2019-ncov-eueea (19 March 2021, date last accessed)
-
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020; 323: 1239–1242 - PubMed
