

PRODIGY: A Phase III Study of Neoadjuvant Docetaxel, Oxaliplatin, and S-1 Plus Surgery and Adjuvant S-1 Versus Surgery and Adjuvant S-1 for Resectable Advanced Gastric Cancer
- PMID: 34133211
- PMCID: PMC8425847
- DOI: 10.1200/JCO.20.02914
PRODIGY: A Phase III Study of Neoadjuvant Docetaxel, Oxaliplatin, and S-1 Plus Surgery and Adjuvant S-1 Versus Surgery and Adjuvant S-1 for Resectable Advanced Gastric Cancer
Abstract
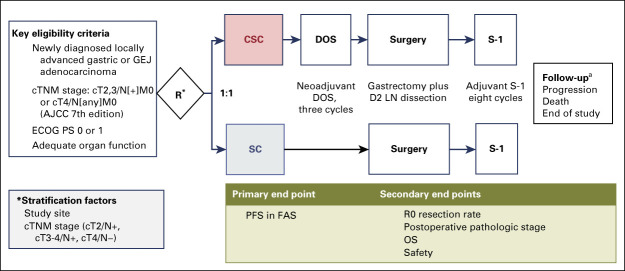
Purpose: Adjuvant chemotherapy after D2 gastrectomy is standard for resectable locally advanced gastric cancer (LAGC) in Asia. Based on positive findings for perioperative chemotherapy in European phase III studies, the phase III PRODIGY study (ClinicalTrials.gov identifier: NCT01515748) investigated whether neoadjuvant docetaxel, oxaliplatin, and S-1 (DOS) followed by surgery and adjuvant S-1 could improve outcomes versus standard treatment in Korean patients with resectable LAGC.
Patients and methods: Patients 20-75 years of age, with Eastern Cooperative Oncology Group performance status 0-1, and with histologically confirmed primary gastric or gastroesophageal junction adenocarcinoma (clinical TNM staging: T2-3N+ or T4Nany) were randomly assigned to D2 surgery followed by adjuvant S-1 (40-60 mg orally twice a day, days 1-28 every 6 weeks for eight cycles; SC group) or neoadjuvant DOS (docetaxel 50 mg/m2, oxaliplatin 100 mg/m2 intravenously day 1, S-1 40 mg/m2 orally twice a day, days 1-14 every 3 weeks for three cycles) before D2 surgery, followed by adjuvant S-1 (CSC group). The primary objective was progression-free survival (PFS) with CSC versus SC. Two sensitivity analyses were performed: intent-to-treat and landmark PFS analysis.
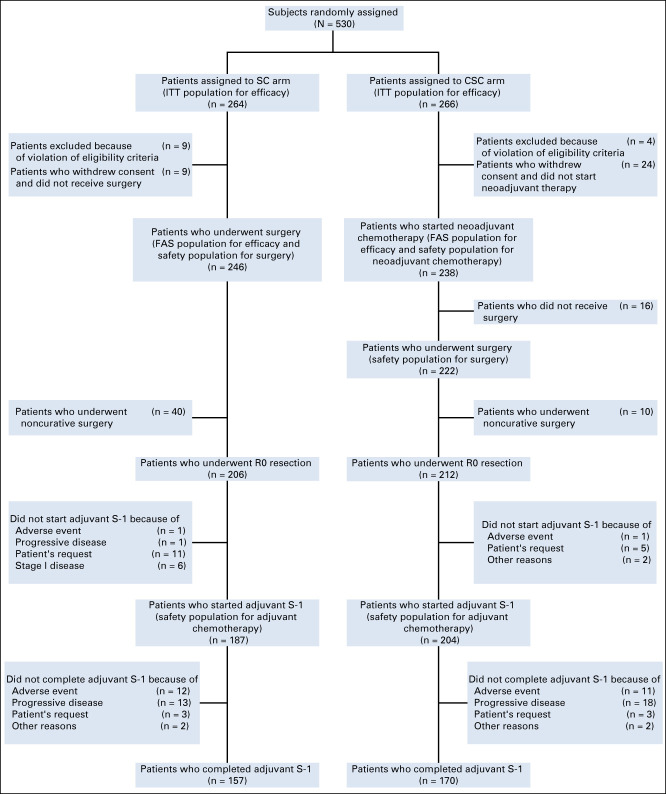
Results: Between January 18, 2012, and January 2, 2017, 266 patients were randomly assigned to CSC and 264 to SC at 18 Korean study sites; 238 and 246 patients, respectively, were treated (full analysis set). Follow-up was ongoing in 176 patients at data cutoff (January 21, 2019; median follow-up 38.6 months [interquartile range, 23.5-62.1]). CSC improved PFS versus SC (adjusted hazard ratio, 0.70; 95% CI, 0.52 to 0.95; stratified log-rank P = .023). Sensitivity analyses confirmed these findings. Treatments were well tolerated. Two grade 5 adverse events (febrile neutropenia and dyspnea) occurred during neoadjuvant treatment.
Conclusion: PRODIGY showed that neoadjuvant DOS chemotherapy, as part of perioperative chemotherapy, is effective and tolerable in Korean patients with LAGC.
Conflict of interest statement
Figures




Comment in
-
Reply to D.-C. Mo et al.J Clin Oncol. 2021 Dec 1;39(34):3884-3886. doi: 10.1200/JCO.21.02043. Epub 2021 Sep 30. J Clin Oncol. 2021. PMID: 34591598 No abstract available.
-
Neoadjuvant Docetaxel, Oxaliplatin, and S-1 in Resectable Advanced Gastric Cancer.J Clin Oncol. 2021 Dec 1;39(34):3883-3884. doi: 10.1200/JCO.21.01528. Epub 2021 Sep 30. J Clin Oncol. 2021. PMID: 34591655 No abstract available.
References
-
- Bang YJ Kim YW Yang HK, et al. : Adjuvant capecitabine and oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): Phase 3 open-label, randomised controlled trial. Lancet 379:315-321, 2012 - PubMed
-
- Cunningham D Allum WH Stenning SP, et al. : Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med 355:11-20, 2006 - PubMed
-
- Macdonald JS Smalley SR Benedetti J, et al. : Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N Engl J Med 345:725-730, 2001 - PubMed
-
- Sakuramoto S Sasako M Yamaguchi T, et al. : Adjuvant chemotherapy for gastric cancer with S-1, an oral fluoropyrimidine. N Engl J Med 357:1810-1820, 2007 - PubMed
-
- Cunningham D Stenning SP Smyth EC, et al. : Peri-operative chemotherapy with or without bevacizumab in operable oesophagogastric adenocarcinoma (UK Medical Research Council ST03): Primary analysis results of a multicentre, open-label, randomised phase 2-3 trial. Lancet Oncol 18:357-370, 2017 - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
