

Predictive performance of critical illness scores and procalcitonin in sepsis caused by different gram-stain bacteria
- PMID: 34133658
- PMCID: PMC8158675
- DOI: 10.6061/clinics/2021/e2610
Predictive performance of critical illness scores and procalcitonin in sepsis caused by different gram-stain bacteria
Abstract
Objectives: To compare the early and late predictive values of several critical illness scores (CISs) and biomarkers in sepsis-3 patients with bloodstream infections (BSIs) and to identify the prognostic value of procalcitonin (PCT) for different gram-stain bacteria infections.
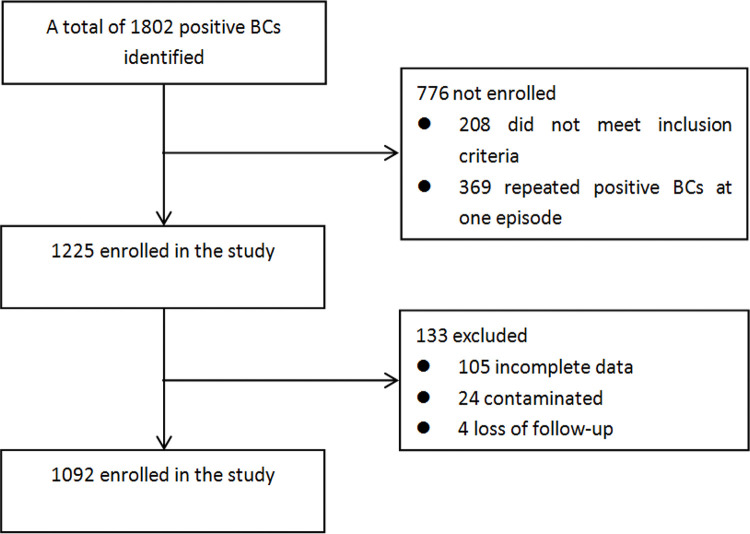
Methods: Patients with at least one positive blood culture within 24h of emergency department admission and with a final diagnosis of sepsis/septic shock were enrolled. CISs were calculated based on the first parameters on the day of admission. The receiver operating characteristics curve was used to analyze the predictive value of CISs and biomarkers for early and late mortality.
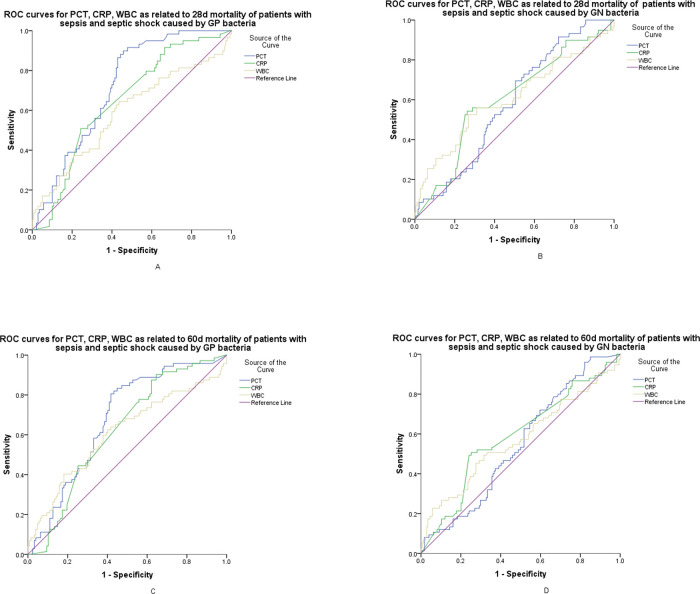
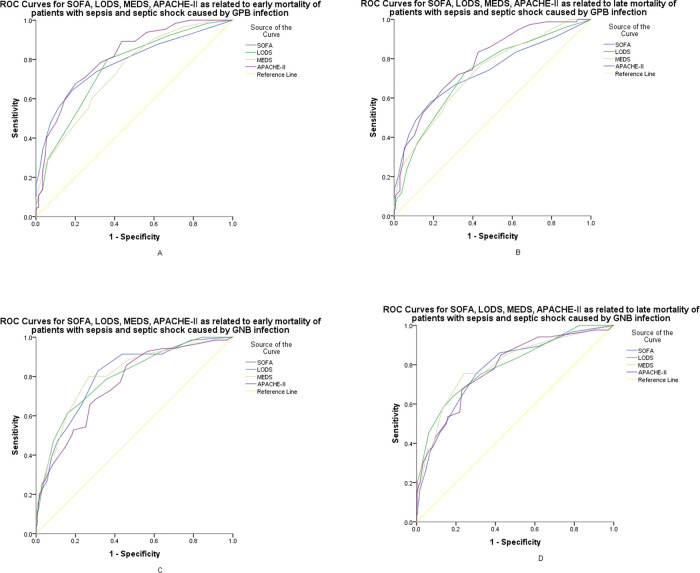
Results: Of 834 enrolled patients with sepsis-3, death occurred in 214 patients within 28 days and in 273 patients within 60 days. Compared with biomarkers, CISs showed a significantly higher area under the curve (AUC) in the prediction of early and late mortality (p<0.01), especially for patients with GNB infection. The Sequential Organ Failure Assessment score showed a higher AUC for predicting early mortality than the Mortality in Emergency Department Sepsis score (p=0.036). Compared with GNB infections, the AUC values of the PCT for gram-positive bacteria (GPB) infections were higher for predicting early or late mortality; PCT showed higher AUC than high-sensitivity C-reactive protein and white blood cells for predicting early mortality (p<0.05).
Conclusions: CISs were more advantageous in the assessment of early and late prognosis, especially for patients with GNB infections; however, for sepsis with GPB infection, PCT can be used for the prediction of early mortality.
Conflict of interest statement
No potential conflict of interest was reported.
Figures

Similar articles
-
[Diagnostic and predictive value of critical illness scores and biomarkers in bloodstream infection-associated pneumonia].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020 Jun;32(6):681-685. doi: 10.3760/cma.j.cn121430-20200428-00345. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020. PMID: 32684212 Chinese.
-
[Value of procalcitonin and critical illness score in etiological diagnosis and prognosis of sepsis caused by intra-abdominal infections].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021 Jul;33(7):792-797. doi: 10.3760/cma.j.cn121430-20200909-00621. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021. PMID: 34412746 Chinese.
-
[Combined prognostic value of serum lactic acid, procalcitonin and severity score for short-term prognosis of septic shock patients].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021 Mar;33(3):281-285. doi: 10.3760/cma.j.cn121430-20201113-00715. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021. PMID: 33834968 Chinese.
-
Advances and Challenges in Pediatric Sepsis Diagnosis: Integrating Early Warning Scores and Biomarkers for Improved Prognosis.Biomolecules. 2025 Jan 14;15(1):123. doi: 10.3390/biom15010123. Biomolecules. 2025. PMID: 39858517 Free PMC article. Review.
-
Usefulness of monocyte distribution width (MDW) as a sepsis biomarker.Rev Esp Quimioter. 2022 Apr;35 Suppl 1(Suppl 1):2-5. doi: 10.37201/req/s01.01.2022. Epub 2022 Apr 22. Rev Esp Quimioter. 2022. PMID: 35488816 Free PMC article. Review.
Cited by
-
Epidemiology and Risk Factors of Community-Associated Bloodstream Infections in Zhejiang Province, China, 2017-2020.Infect Drug Resist. 2023 Mar 18;16:1579-1590. doi: 10.2147/IDR.S400108. eCollection 2023. Infect Drug Resist. 2023. PMID: 36969944 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
