

Inter-rater reliability and prospective validation of a clinical prediction rule for SARS-CoV-2 infection
- PMID: 34133794
- PMCID: PMC8441807
- DOI: 10.1111/acem.14309
Inter-rater reliability and prospective validation of a clinical prediction rule for SARS-CoV-2 infection
Abstract
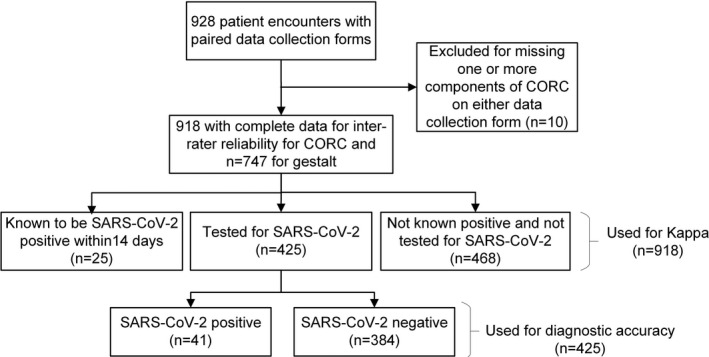
Objectives: Accurate estimation of the risk of SARS-CoV-2 infection based on bedside data alone has importance to emergency department (ED) operations and throughput. The 13-item CORC (COVID [or coronavirus] Rule-out Criteria) rule had good overall diagnostic accuracy in retrospective derivation and validation. The objective of this study was to prospectively test the inter-rater reliability and diagnostic accuracy of the CORC score and rule (score ≤ 0 negative, > 0 positive) and compare the CORC rule performance with physician gestalt.
Methods: This noninterventional study was conducted at an urban academic ED from February 2021 to March 2021. Two practitioners were approached by research coordinators and asked to independently complete a form capturing the CORC criteria for their shared patient and their gestalt binary prediction of the SARS-CoV-2 test result and confidence (0%-100%). The criterion standard for SARS-CoV-2 was from reverse transcriptase polymerase chain reaction performed on a nasopharyngeal swab. The primary analysis was from weighted Cohen's kappa and likelihood ratios (LRs).
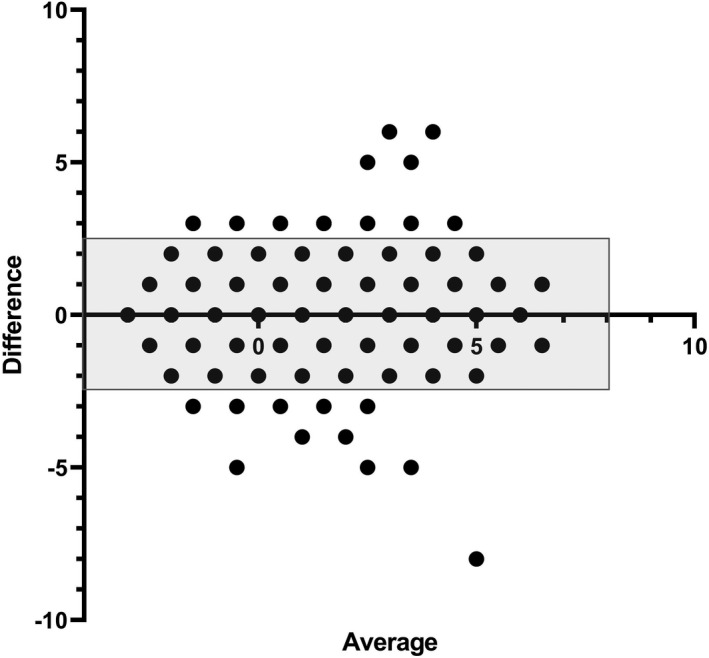
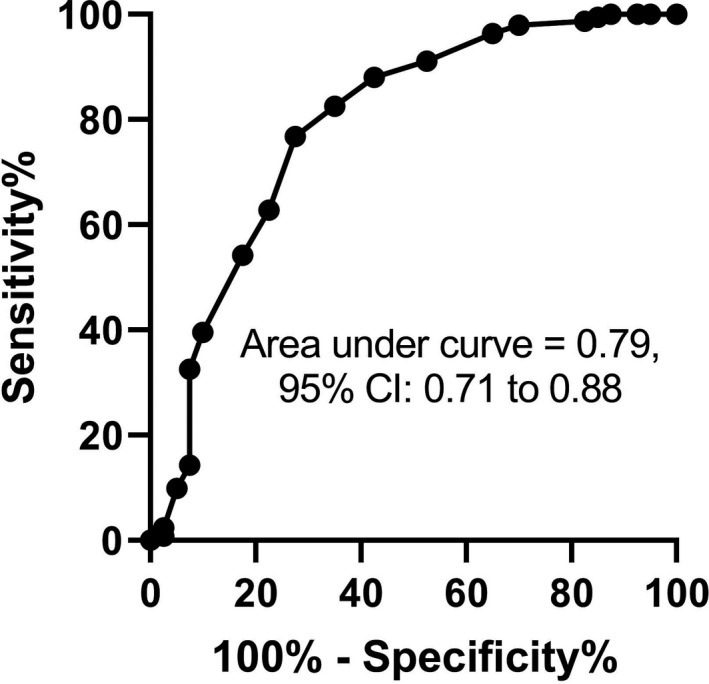
Results: For 928 patients, agreement between observers was good for the total CORC score, κ = 0.613 (95% confidence interval [CI] = 0.579-0.646), and for the CORC rule, κ = 0.644 (95% CI = 0.591-0.697). The agreement for clinician gestalt binary determination of SARs-CoV-2 status was κ = 0.534 (95% CI = 0.437-0.632) with median confidence of 76% (first-third quartile = 66-88.5). For 425 patients who had the criterion standard, a negative CORC rule (both observers scored CORC < 0), the sensitivity was 88%, and specificity was 51%, with a negative LR (LR-) of 0.24 (95% CI = 0.10-0.50). Among patients with a mean CORC score of >4, the prevalence of a positive SARS-CoV-2 test was 58% (95% CI = 28%-85%) and positive LR was 13.1 (95% CI = 4.5-37.2). Clinician gestalt demonstrated a sensitivity of 51% and specificity of 86% with a LR- of 0.57 (95% CI = 0.39-0.74).
Conclusion: In this prospective study, the CORC score and rule demonstrated good inter-rater reliability and reproducible diagnostic accuracy for estimating the pretest probability of SARs-CoV-2 infection.
Keywords: COVID-19; SARS-CoV-2; decision making; diagnosis; multivariable analysis; probability; prognosis; registries; risk.
© 2021 by the Society for Academic Emergency Medicine.
Conflict of interest statement
The authors have no potential conflicts to disclose.
Figures
Similar articles
-
Clinical prediction rule for SARS-CoV-2 infection from 116 U.S. emergency departments 2-22-2021.PLoS One. 2021 Mar 10;16(3):e0248438. doi: 10.1371/journal.pone.0248438. eCollection 2021. PLoS One. 2021. PMID: 33690722 Free PMC article.
-
A Rapid Antigen Detection Test to Diagnose SARS-CoV-2 Infection Using Exhaled Breath Condensate by A Modified Inflammacheck® Device.Sensors (Basel). 2021 Aug 25;21(17):5710. doi: 10.3390/s21175710. Sensors (Basel). 2021. PMID: 34502603 Free PMC article.
-
Diagnostic accuracy of physician's gestalt in suspected COVID-19: Prospective bicentric study.Acad Emerg Med. 2021 Apr;28(4):404-411. doi: 10.1111/acem.14232. Epub 2021 Mar 15. Acad Emerg Med. 2021. PMID: 33576155 Free PMC article.
-
Thoracic imaging tests for the diagnosis of COVID-19.Cochrane Database Syst Rev. 2020 Sep 30;9:CD013639. doi: 10.1002/14651858.CD013639.pub2. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2020 Nov 26;11:CD013639. doi: 10.1002/14651858.CD013639.pub3. PMID: 32997361 Updated.
-
Thoracic imaging tests for the diagnosis of COVID-19.Cochrane Database Syst Rev. 2020 Nov 26;11:CD013639. doi: 10.1002/14651858.CD013639.pub3. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2021 Mar 16;3:CD013639. doi: 10.1002/14651858.CD013639.pub4. PMID: 33242342 Updated.
Cited by
-
CCEDRRN COVID-19 Infection Score (CCIS): development and validation in a Canadian cohort of a clinical risk score to predict SARS-CoV-2 infection in patients presenting to the emergency department with suspected COVID-19.BMJ Open. 2021 Dec 2;11(12):e055832. doi: 10.1136/bmjopen-2021-055832. BMJ Open. 2021. PMID: 34857584 Free PMC article.
References
-
- Kurstjens S, van der Horst A , Herpers R, et al. Rapid identification of SARS‐CoV‐2‐infected patients at the emergency department using routine testing. Clin Chem Lab Med. 2020;58(9):1587‐1593. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
