

Sudden Cardiac Death and Myocardial Fibrosis, Determined by Autopsy, in Persons with HIV
- PMID: 34133860
- PMCID: PMC8415173
- DOI: 10.1056/NEJMoa1914279
Sudden Cardiac Death and Myocardial Fibrosis, Determined by Autopsy, in Persons with HIV
Abstract
Background: The incidence of sudden cardiac death and sudden death caused by arrhythmia, as determined by autopsy, in persons with human immunodeficiency virus (HIV) infection has not been clearly established.
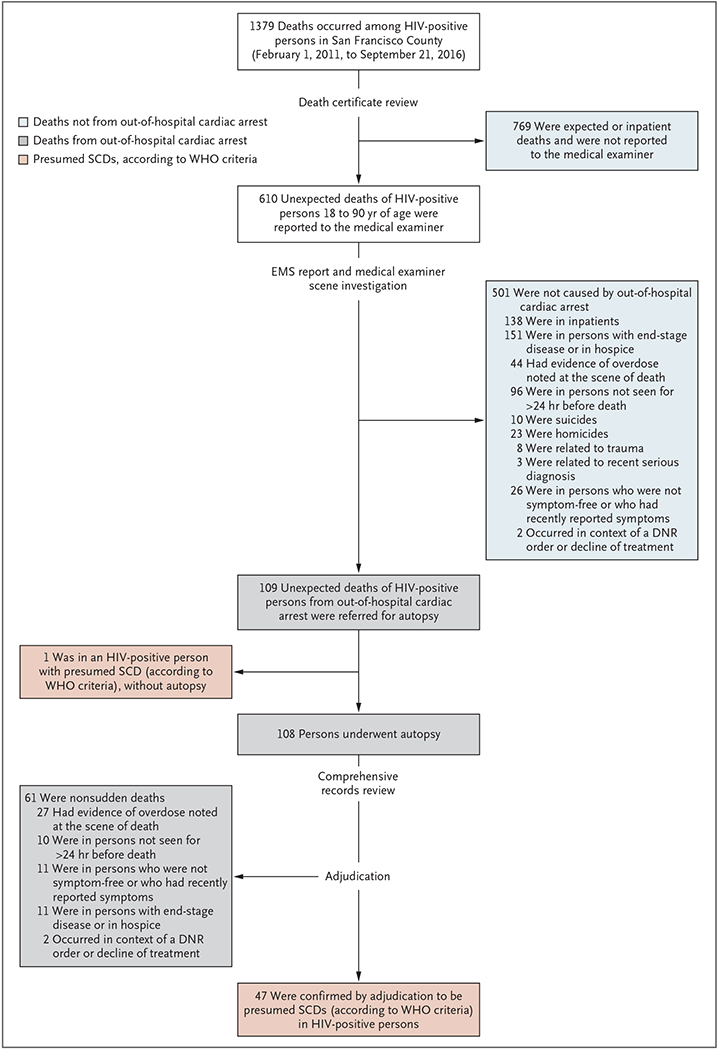
Methods: Between February 1, 2011, and September 16, 2016, we prospectively identified all new deaths due to out-of-hospital cardiac arrest among persons 18 to 90 years of age, with or without known HIV infection, for comprehensive autopsy and toxicologic and histologic testing. We compared the rates of sudden cardiac death and sudden death caused by arrhythmia between groups.
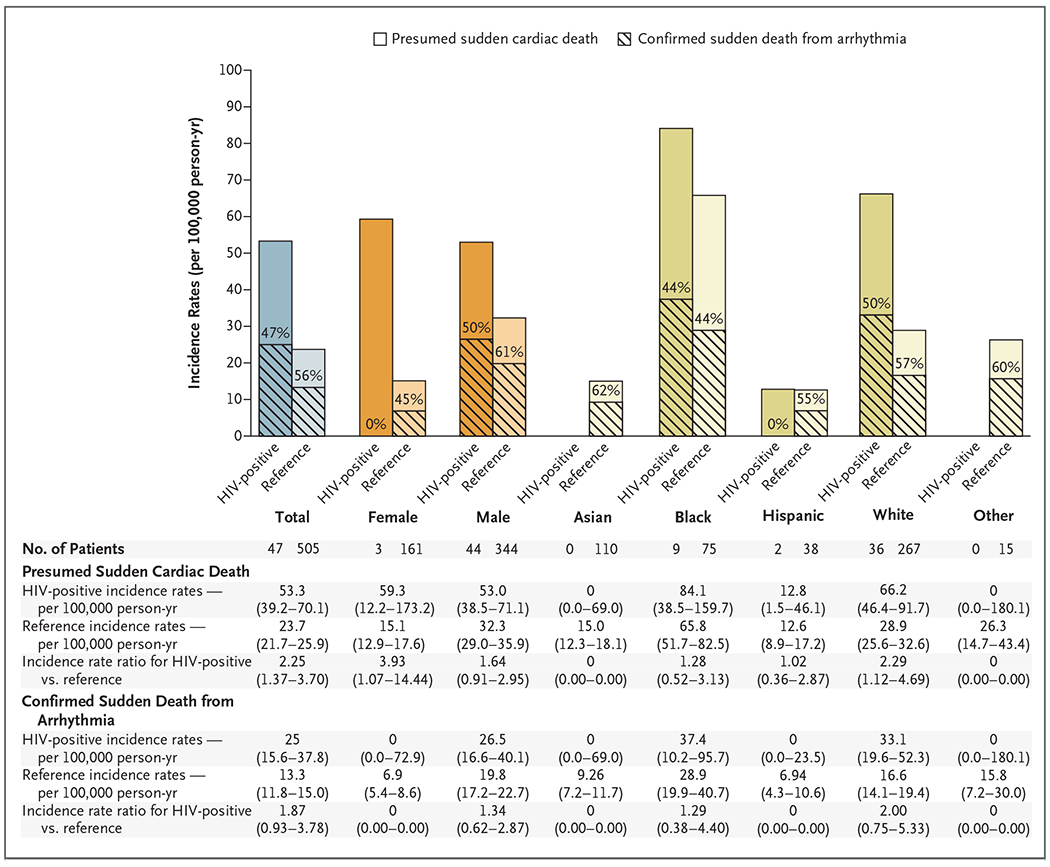
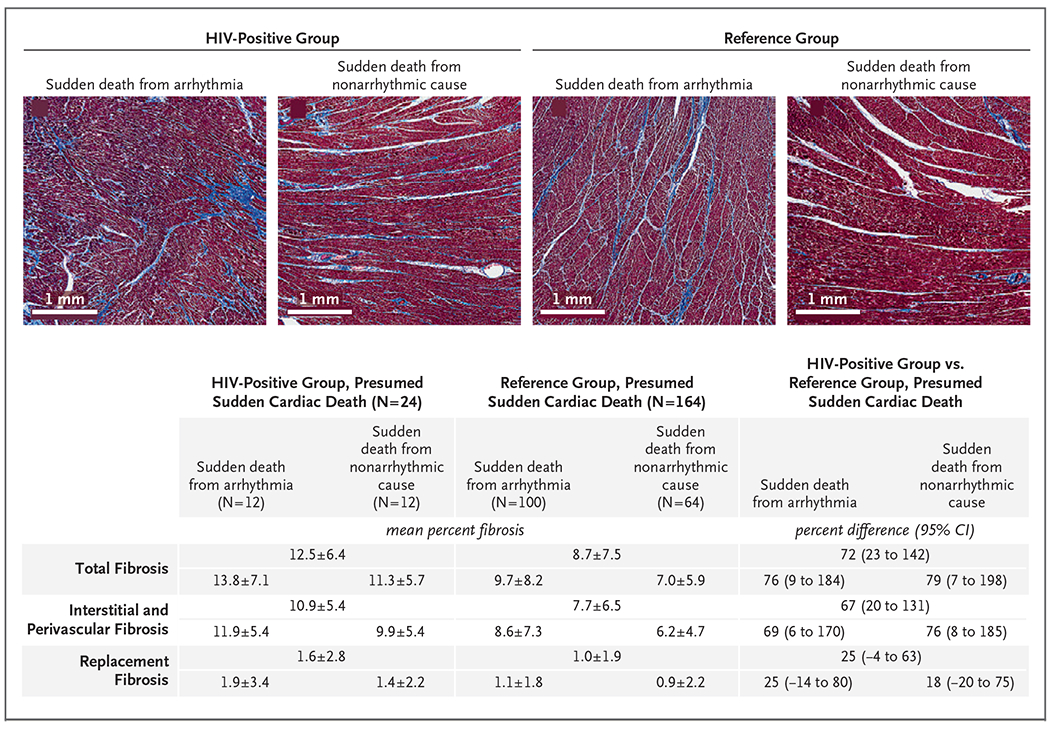
Results: Of 109 deaths from out-of-hospital cardiac arrest among 610 unexpected deaths in HIV-positive persons, 48 met World Health Organization criteria for presumed sudden cardiac death; of those, fewer than half (22) had an arrhythmic cause. A total of 505 presumed sudden cardiac deaths occurred between February 1, 2011, and March 1, 2014, in persons without known HIV infection. Observed incidence rates of presumed sudden cardiac death were 53.3 deaths per 100,000 person-years among persons with known HIV infection and 23.7 deaths per 100,000 person-years among persons without known HIV infection (incidence rate ratio, 2.25; 95% confidence interval [CI], 1.37 to 3.70). Observed incidence rates of sudden death caused by arrhythmia were 25.0 and 13.3 deaths per 100,000 person-years, respectively (incidence rate ratio, 1.87; 95% CI, 0.93 to 3.78). Among all presumed sudden cardiac deaths, death due to occult drug overdose was more common in persons with known HIV infection than in persons without known HIV infection (34% vs. 13%). Persons who were HIV-positive had higher histologic levels of interstitial myocardial fibrosis than persons without known HIV infection.
Conclusions: In this postmortem study, the rates of presumed sudden cardiac death and myocardial fibrosis were higher among HIV-positive persons than among those without known HIV infection. One third of apparent sudden cardiac deaths in HIV-positive persons were due to occult drug overdose. (Supported by the National Heart, Lung, and Blood Institute.).
Copyright © 2021 Massachusetts Medical Society.
Figures
Comment in
-
Sudden Cardiac Death and Myocardial Fibrosis in Persons with HIV.N Engl J Med. 2021 Oct 7;385(15):e50. doi: 10.1056/NEJMc2112481. N Engl J Med. 2021. PMID: 34614339 No abstract available.
-
Sudden Cardiac Death and Myocardial Fibrosis in Persons with HIV.N Engl J Med. 2021 Oct 7;385(15):e50. doi: 10.1056/NEJMc2112481. N Engl J Med. 2021. PMID: 34614340 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous