

Seroconversion rates following COVID-19 vaccination among patients with cancer
- PMID: 34133951
- PMCID: PMC8179248
- DOI: 10.1016/j.ccell.2021.06.002
Seroconversion rates following COVID-19 vaccination among patients with cancer
Abstract
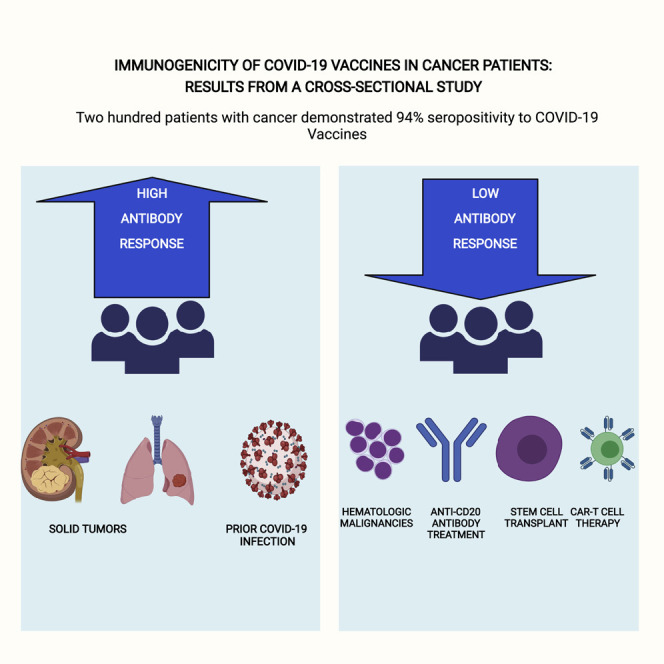
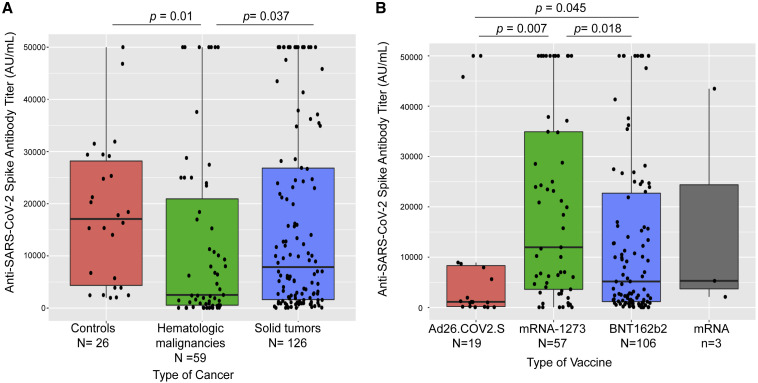
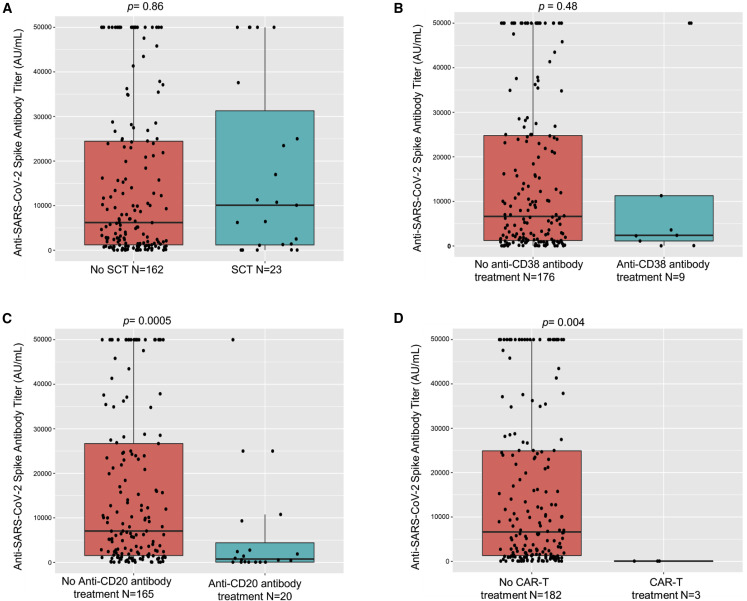
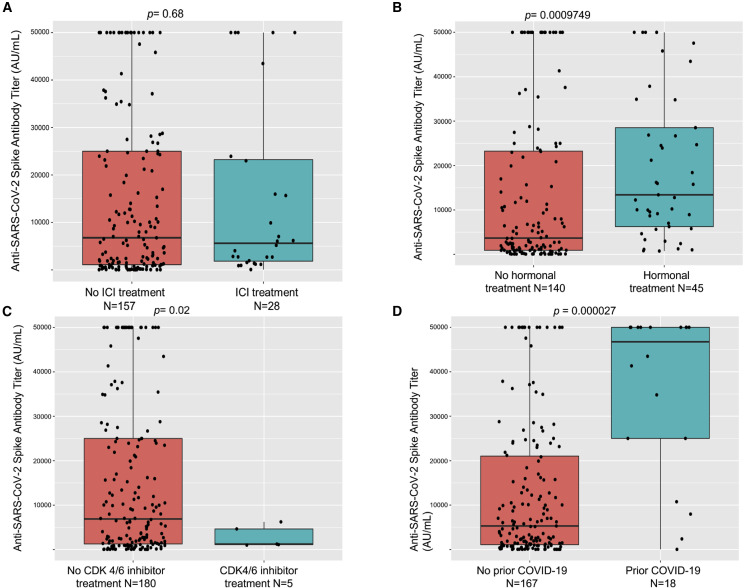
As COVID-19 adversely affects patients with cancer, prophylactic strategies are critically needed. Using a validated antibody assay against SARS-CoV-2 spike protein, we determined a high seroconversion rate (94%) in 200 patients with cancer in New York City that had received full dosing with one of the FDA-approved COVID-19 vaccines. On comparison with solid tumors (98%), a significantly lower rate of seroconversion was observed in patients with hematologic malignancies (85%), particularly recipients following highly immunosuppressive therapies such as anti-CD20 therapies (70%) and stem cell transplantation (73%). Patients receiving immune checkpoint inhibitor therapy (97%) or hormonal therapies (100%) demonstrated high seroconversion post vaccination. Patients with prior COVID-19 infection demonstrated higher anti-spike IgG titers post vaccination. Relatively lower IgG titers were observed following vaccination with the adenoviral than with mRNA-based vaccines. These data demonstrate generally high immunogenicity of COVID-19 vaccination in oncology patients and identify immunosuppressed cohorts that need novel vaccination or passive immunization strategies.
Keywords: COVID-19; cancer; hematologi malignancies; vaccine.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests A.V. has received research funding from GlaxoSmithKline, BMS, Janssen, Incyte, MedPacto, Celgene, Novartis, Curis, Prelude, and Eli Lilly and Company, has received compensation as a scientific advisor to Novartis, Stelexis Therapeutics, Acceleron Pharma, and Celgene, and has equity ownership in Stelexis Therapeutics. All other authors declare no competing interests.
Figures
Comment in
-
Immunogenicity of a heterologous COVID-19 vaccine after failed vaccination in a lymphoma patient.Cancer Cell. 2021 Aug 9;39(8):1037-1038. doi: 10.1016/j.ccell.2021.06.015. Epub 2021 Jun 26. Cancer Cell. 2021. PMID: 34242571 Free PMC article. No abstract available.
-
Highly variable SARS-CoV-2 spike antibody responses to two doses of COVID-19 RNA vaccination in patients with multiple myeloma.Cancer Cell. 2021 Aug 9;39(8):1028-1030. doi: 10.1016/j.ccell.2021.06.014. Epub 2021 Jun 29. Cancer Cell. 2021. PMID: 34242572 Free PMC article. No abstract available.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
