

Clinical features and predictors of masked uncontrolled hypertension from the Korean Ambulatory Blood Pressure Monitoring Registry
- PMID: 34134467
- PMCID: PMC8435491
- DOI: 10.3904/kjim.2020.650
Clinical features and predictors of masked uncontrolled hypertension from the Korean Ambulatory Blood Pressure Monitoring Registry
Abstract
Background/aims: The clinical characteristics of patients with masked uncontrolled hypertension (MUCH) have been poorly defined, and few studies have investigated the clinical predictors of MUCH. We investigated the demographic, clinical, and blood pressure (BP) characteristics of patients with MUCH and proposed a prediction model for MUCH in patients with hypertension.
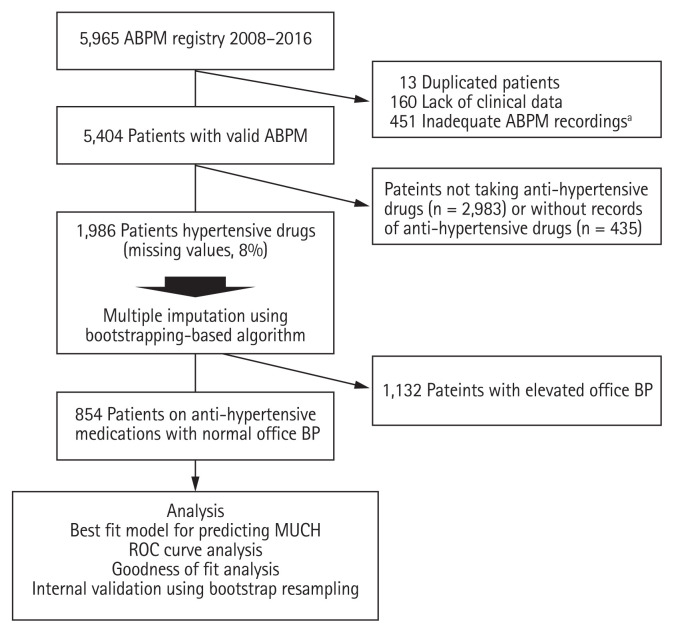
Methods: We analyzed 1,986 subjects who were enrolled in the Korean Ambulatory Blood Pressure Monitoring (Kor-ABP) Registry and taking antihypertensive drugs, and classified them into the controlled hypertension (n = 465) and MUCH (n = 389) groups. MUCH was defined as the presence of a 24-hour ambulatory mean systolic BP ≥ 130 mmHg and/or diastolic BP ≥ 80 mmHg in patients treated with antihypertensive drugs, having normal office BP.
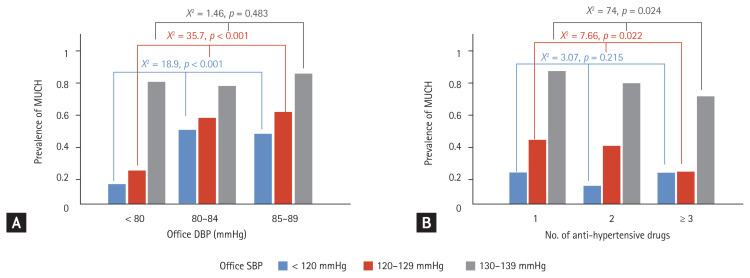
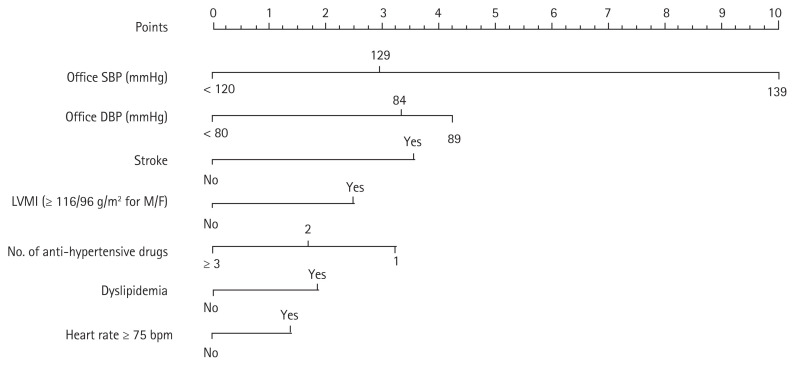
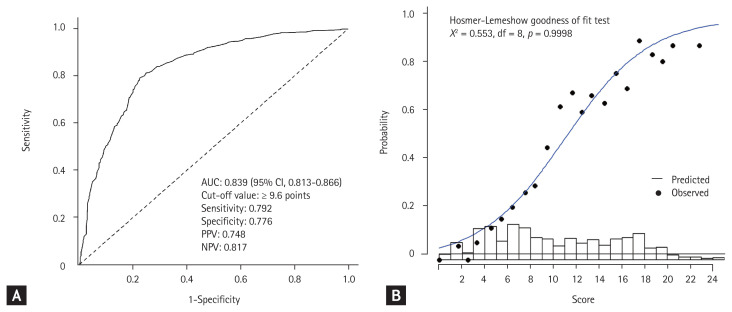
Results: Patients in the MUCH group had significantly worse metabolic profiles and higher office BP, and took significantly fewer antihypertensive drugs compared to those in the controlled hypertension group. Multivariate logistic regression analyses identified high office systolic BP and diastolic BP, prior stroke, dyslipidemia, left ventricular hypertrophy (LVH, ≥ 116 g/m2 for men, and ≥ 96 g/m2 for women), high heart rate (≥ 75 beats/min), and single antihypertensive drug use as independent predictors of MUCH. A prediction model using these predictors showed a high diagnostic accuracy (C-index of 0.839) and goodness-of-fit for the presence of MUCH.
Conclusion: MUCH is associated with a high-normal increase in office BP and underuse of antihypertensive drugs, as well as dyslipidemia, prior stroke, and LVH, which could underscore achieving optimal BP control. The proposed model accurately predicts MUCH in patients with controlled office BP.
Keywords: Blood pressure; Blood pressure monitoring, ambulatory; Masked uncontrolled hypertension.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Impact of Clinic Blood Pressure Target on the Prevalence and Predictors of Masked Uncontrolled Hypertension and White-Coat Uncontrolled Hypertension.J Korean Med Sci. 2025 Jun 23;40(24):e117. doi: 10.3346/jkms.2025.40.e117. J Korean Med Sci. 2025. PMID: 40551606 Free PMC article.
-
Blood Pressure Control in Hypertensive Patients, Cardiovascular Risk Profile and the Prevalence of Masked Uncontrolled Hypertension (MUCH).Med Arch. 2016 Jul 27;70(4):274-279. doi: 10.5455/medarh.2016.70.274-279. Med Arch. 2016. PMID: 27703288 Free PMC article.
-
Prevalence and Characteristics of Isolated Nighttime Masked Uncontrolled Hypertension in Treated Patients.Medicina (Kaunas). 2024 Sep 18;60(9):1522. doi: 10.3390/medicina60091522. Medicina (Kaunas). 2024. PMID: 39336563 Free PMC article.
-
The complexity of masked hypertension: diagnostic and management challenges.Curr Hypertens Rep. 2014 Sep;16(9):474. doi: 10.1007/s11906-014-0474-4. Curr Hypertens Rep. 2014. PMID: 25097111 Review.
-
Ambulatory blood pressure monitoring in daily clinical practice - the Spanish ABPM Registry experience.Eur J Clin Invest. 2016 Jan;46(1):92-8. doi: 10.1111/eci.12565. Epub 2015 Dec 23. Eur J Clin Invest. 2016. PMID: 26541761 Review.
Cited by
-
DCRM Multispecialty Practice Recommendations for the management of diabetes, cardiorenal, and metabolic diseases.J Diabetes Complications. 2022 Feb;36(2):108101. doi: 10.1016/j.jdiacomp.2021.108101. Epub 2021 Dec 7. J Diabetes Complications. 2022. PMID: 34922811 Free PMC article. Review.
-
Nomogram based on clinical features at a single outpatient visit to predict masked hypertension and masked uncontrolled hypertension: A study of diagnostic accuracy.Medicine (Baltimore). 2022 Dec 9;101(49):e32144. doi: 10.1097/MD.0000000000032144. Medicine (Baltimore). 2022. PMID: 36626526 Free PMC article.
-
Clinical and life style factors related to the nighttime blood pressure, nighttime dipping and their phenotypes in Korean hypertensive patients.Clin Hypertens. 2023 Aug 1;29(1):21. doi: 10.1186/s40885-023-00241-w. Clin Hypertens. 2023. PMID: 37525293 Free PMC article.
-
The 2022 focused update of the 2018 Korean Hypertension Society Guidelines for the management of hypertension.Clin Hypertens. 2023 Feb 15;29(1):11. doi: 10.1186/s40885-023-00234-9. Clin Hypertens. 2023. PMID: 36788612 Free PMC article. Review.
-
When and how to use ambulatory blood pressure monitoring and home blood pressure monitoring for managing hypertension.Clin Hypertens. 2024 Apr 1;30(1):10. doi: 10.1186/s40885-024-00265-w. Clin Hypertens. 2024. PMID: 38556887 Free PMC article. Review.
References
-
- Banegas JR, Ruilope LM, de la Sierra A, et al. High prevalence of masked uncontrolled hypertension in people with treated hypertension. Eur Heart J. 2014;35:3304–3312. - PubMed
-
- Franklin SS, O’Brien E, Staessen JA. Masked hypertension: understanding its complexity. Eur Heart J. 2017;38:1112–1118. - PubMed
-
- Franklin SS, O’Brien E, Thijs L, Asayama K, Staessen JA. Masked hypertension: a phenomenon of measurement. Hypertension. 2015;65:16–20. - PubMed
-
- Ohkubo T, Kikuya M, Metoki H, et al. Prognosis of “masked” hypertension and “white-coat” hypertension detected by 24-h ambulatory blood pressure monitoring 10-year follow-up from the Ohasama study. J Am Coll Cardiol. 2005;46:508–515. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical