

Effect of Medical and Surgical Interventions on α-Cell Function in Dysglycemic Youth and Adults in the RISE Study
- PMID: 34135015
- PMCID: PMC8740921
- DOI: 10.2337/dc21-0461
Effect of Medical and Surgical Interventions on α-Cell Function in Dysglycemic Youth and Adults in the RISE Study
Abstract
Objective: To compare effects of medications and laparoscopic gastric band surgery (LB) on α-cell function in dysglycemic youth and adults in the Restoring Insulin Secretion (RISE) Study protocols.
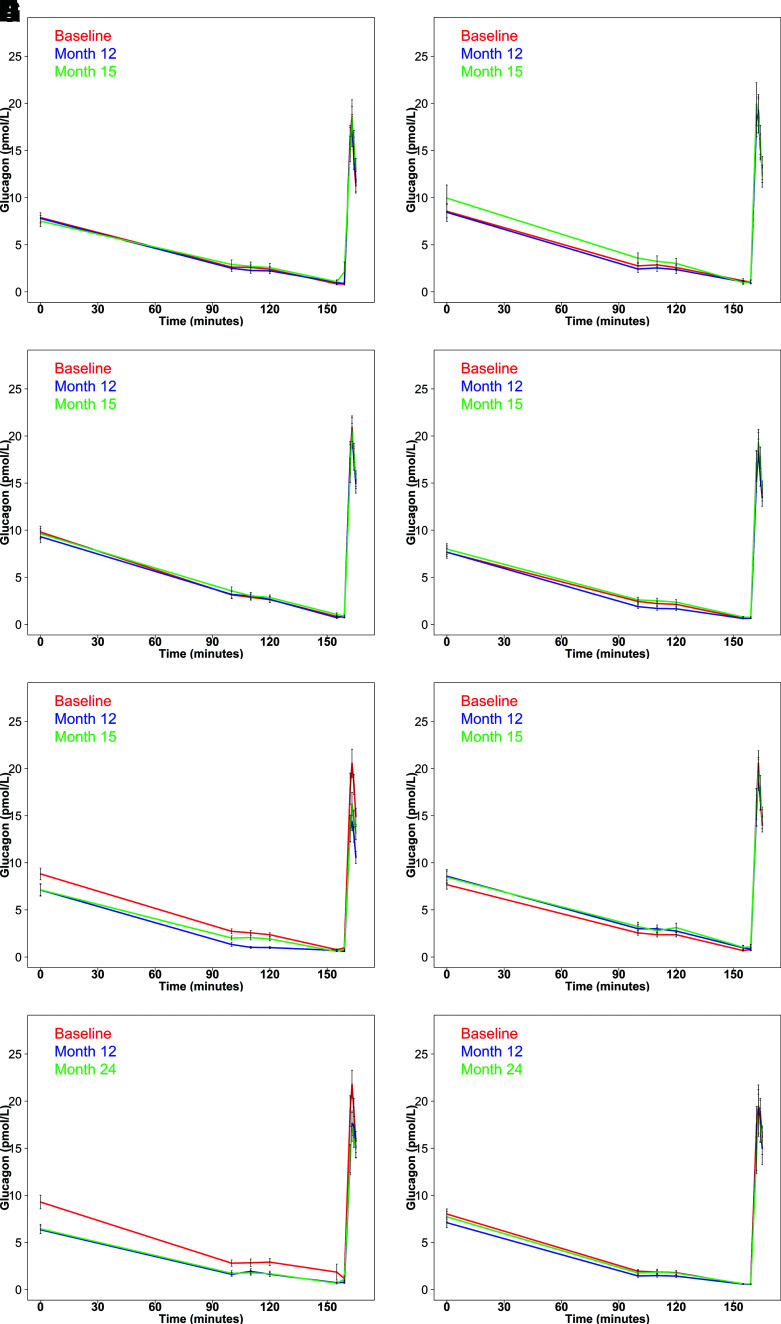
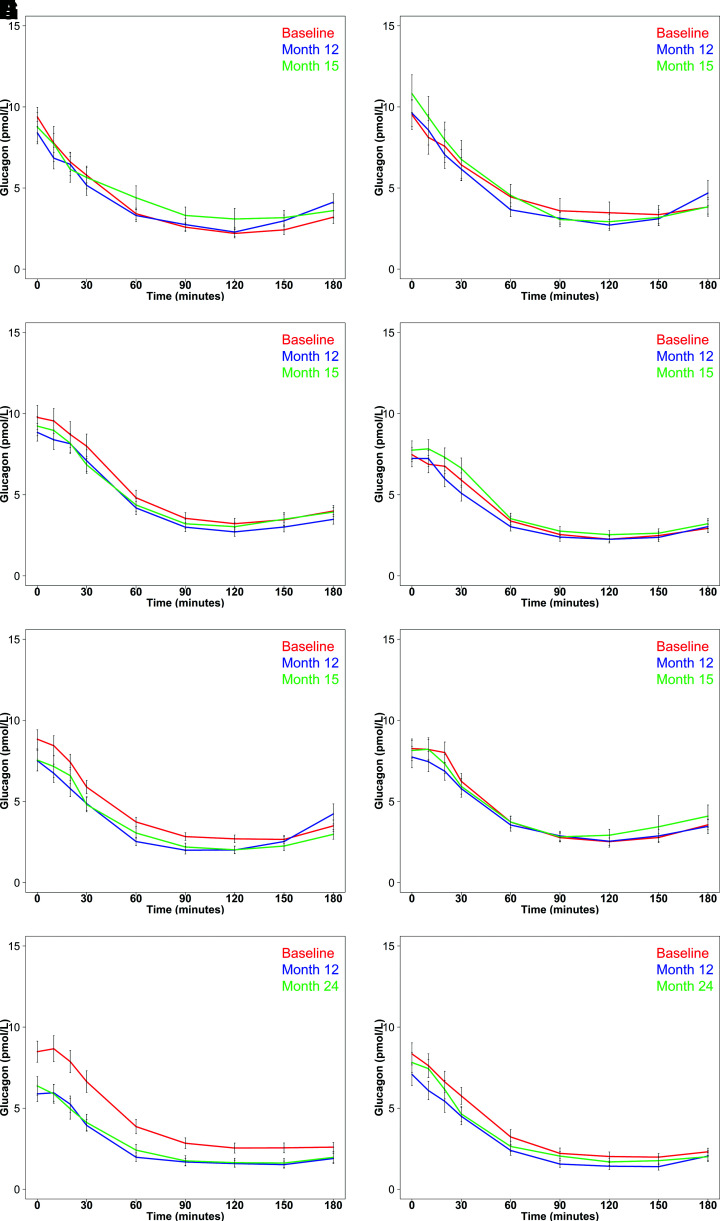
Research design and methods: Glucagon was measured in three randomized, parallel, clinical studies: 1) 91 youth studied at baseline, after 12 months on metformin alone (MET) or glargine followed by metformin (G/M), and 3 months after treatment withdrawal; 2) 267 adults studied at the same time points and treated with MET, G/M, or liraglutide plus metformin (L+M) or given placebo (PLAC); and 3) 88 adults studied at baseline and after 12 and 24 months of LB or MET. Fasting glucagon, glucagon suppression by glucose, and acute glucagon response (AGR) to arginine were assessed during hyperglycemic clamps. Glucagon suppression was also measured during oral glucose tolerance tests (OGTTs).
Results: No change in fasting glucagon, steady-state glucagon, or AGR was seen at 12 months following treatment with MET or G/M (in youth and adults) or PLAC (in adults). In contrast, L+M reduced these measures at 12 months (all P ≤ 0.005), which was maintained 3 months after treatment withdrawal (all P < 0.01). LB in adults also reduced fasting glucagon, steady-state glucagon, and AGR at 12 and 24 months (P < 0.05 for all, except AGR at 12 months [P = 0.098]). Similarly, glucagon suppression during OGTTs was greater with L+M and LB. Linear models demonstrated that treatment effects on glucagon with L+M and LB were largely associated with weight loss.
Conclusions: Glucagon concentrations were reduced by L+M and LB in adults with dysglycemia, an effect principally attributable to weight loss in both interventions.
Trial registration: ClinicalTrials.gov NCT01779362 NCT01779375 NCT01763346.
© 2021 by the American Diabetes Association.
Figures
References
-
- Kahn SE, Hull RL, Utzschneider KM. Mechanisms linking obesity to insulin resistance and type 2 diabetes. Nature 2006;444:840–846 - PubMed
-
- Dunning BE, Gerich JE. The role of α-cell dysregulation in fasting and postprandial hyper glycemia in type 2 diabetes and therapeutic implications. Endocr Rev 2007;28:253–283 - PubMed
-
- Ravier MA, Rutter GA. Glucose or insulin, but not zinc ions, inhibit glucagon secretion from mouse pancreatic α-cells. Diabetes 2005;54:1789–1797 - PubMed
-
- Rorsman P, Berggren PO, Bokvist K, et al. Glucose-inhibition of glucagon secretion involves activation of GABAA-receptor chloride channels. Nature 1989;341:233–236 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UL1 TR000430/TR/NCATS NIH HHS/United States
- U01 DK094406/DK/NIDDK NIH HHS/United States
- UL1 TR001857/TR/NCATS NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- U01 DK094431/DK/NIDDK NIH HHS/United States
- U01 DK094430/DK/NIDDK NIH HHS/United States
- P30 DK045735/DK/NIDDK NIH HHS/United States
- UL1 TR001082/TR/NCATS NIH HHS/United States
- P30 DK020595/DK/NIDDK NIH HHS/United States
- P30 DK017047/DK/NIDDK NIH HHS/United States
- TL1 TR001858/TR/NCATS NIH HHS/United States
- UL1 TR001108/TR/NCATS NIH HHS/United States
- U01 DK094438/DK/NIDDK NIH HHS/United States
- P30 DK116073/DK/NIDDK NIH HHS/United States
- U01 DK094467/DK/NIDDK NIH HHS/United States
- P30 DK097512/DK/NIDDK NIH HHS/United States
- K24 HL145076/HL/NHLBI NIH HHS/United States
- UL1 TR001855/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
