

Characteristics and Prognosis of Autoimmune Encephalitis in the East of China: A Multi-Center Study
- PMID: 34135845
- PMCID: PMC8200540
- DOI: 10.3389/fneur.2021.642078
Characteristics and Prognosis of Autoimmune Encephalitis in the East of China: A Multi-Center Study
Abstract
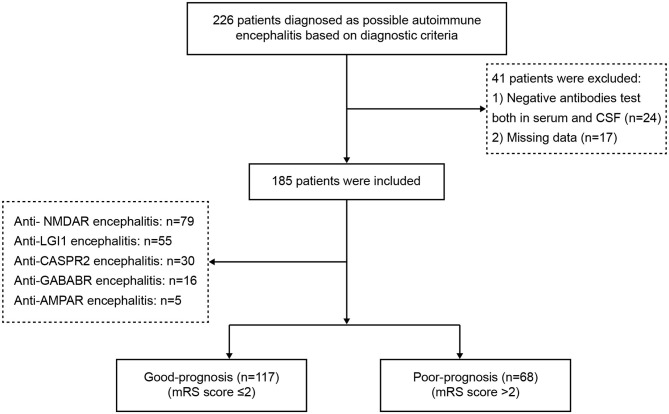
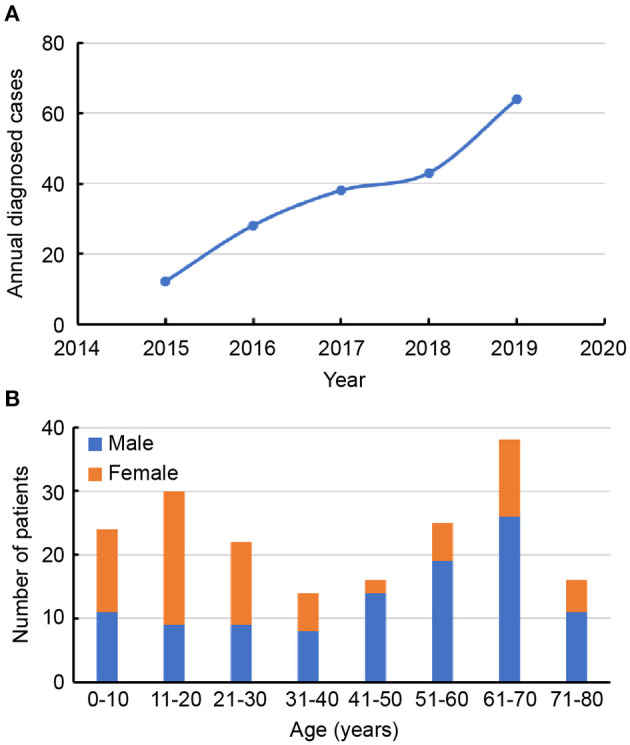
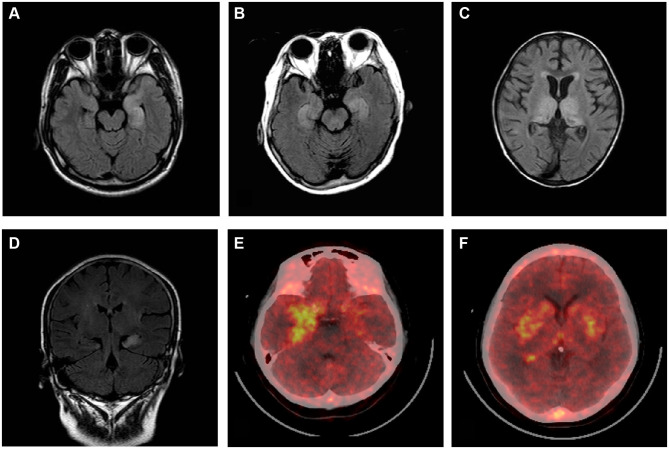
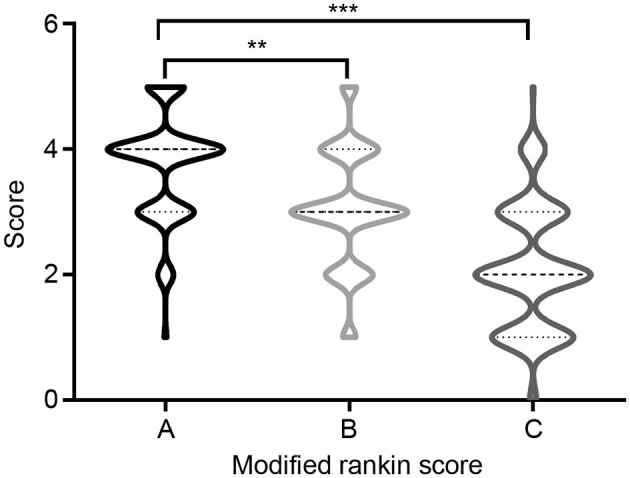
Objective: This study aimed to investigate epidemiological characteristics, clinical manifestations, and long-term outcomes of patients with autoimmune encephalitis (AE) in the east of China. Methods: From January 2015 to December 2019, 226 potential AE patients were recruited from five clinical centers, and a total of 185 patients who met the diagnostic criteria were included in the study. We retrospectively reviewed clinical features, auxiliary examinations, details of treatments, and outcomes of AE, and identified risk factors of poor prognosis. Modified Rankin Scale scores were used to evaluate neurological function, and scores of 3-6 indicated a poor-prognosis. Results: Patients with five main subtypes of AE were enrolled in the study, as follows: anti-NMDAR (79), anti-LGI1 (55), anti-CASPR2 (30), anti-GABABR (16), and anti-AMPAR (5). Among 185 patients, 58.38% (108/185) were male and 41.62% (77/185) were female. The median age at disease onset was 41 years (interquartile range, 17-62). The most common clinical manifestations of AE were seizures (146, 78.92%) and memory deficit (123, 66.49%). A total of 95 (51.35%) patients had abnormal brain magnetic resonance imaging results. Electroencephalographic findings were abnormal in 131 (70.81%) patients, and 168 (90.81%) and 26 (14.05%) patients were treated with first- and second-line immunotherapies, respectively. All surviving patients were followed-up for at least 1 year (range 12-36 months). Good clinical outcomes were achieved in 117 (63.24%), while 68 (36.76%) patients had a poor prognosis. Further, 33 (17.84%) patients relapsed and 10 (5.41%) died within 1 year post-discharge. Older patients tended to have a poorer prognosis, and the occurrence of mental behavioral disorders, movement disorders, disturbance of consciousness, central hypoventilation, and tumors were overrepresented in the poor-prognosis group. Conclusions: AE is a treatable disease, and most patients have a good prognosis. There are differences in the clinical manifestations of patients with different AE subtypes. Some with AE will relapse, and long-term follow-up is of great significance for further research.
Keywords: autoimmune encephalitis; clinical features; epidemiology; prognosis; relapse.
Copyright © 2021 Qiao, Wu, Liu, Zhang, Wang, Han, Zhang and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Endres D, Leypoldt F, Bechter K, Hasan A, Steiner J, Domschke K, et al. . Autoimmune encephalitis as a differential diagnosis of schizophreniform psychosis: clinical symptomatology, pathophysiology, diagnostic approach, therapeutic considerations. Eur Arch Psychiatry Clin Neurosci. (2020) 270:803–18. 10.1007/s00406-020-01113-2 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous