

Risk Stratification Score to Predict Readmission of Patients With Acute Decompensated Cirrhosis Within 90 Days
- PMID: 34136498
- PMCID: PMC8200567
- DOI: 10.3389/fmed.2021.646875
Risk Stratification Score to Predict Readmission of Patients With Acute Decompensated Cirrhosis Within 90 Days
Abstract
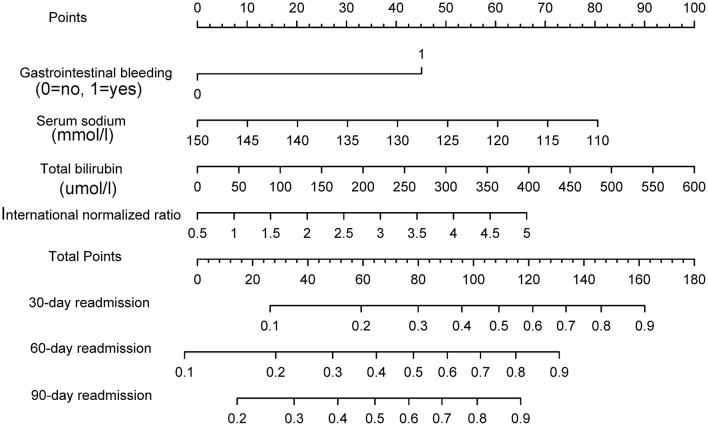
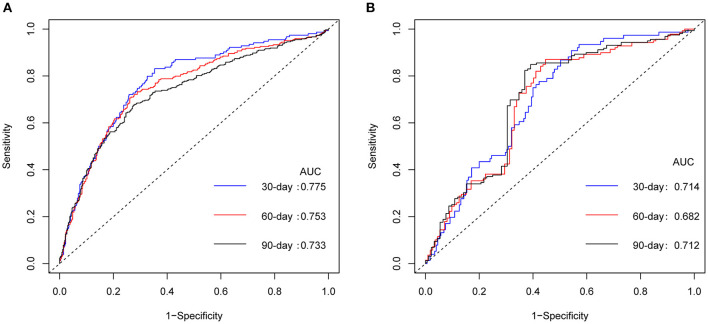
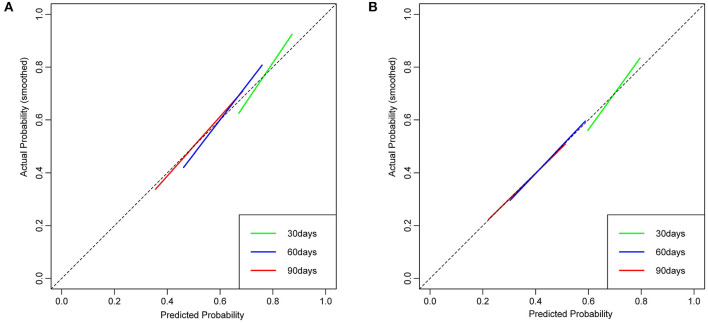
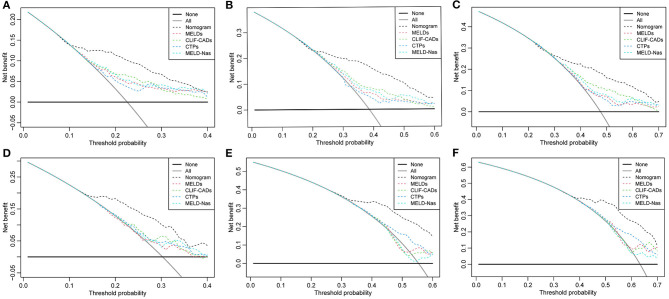
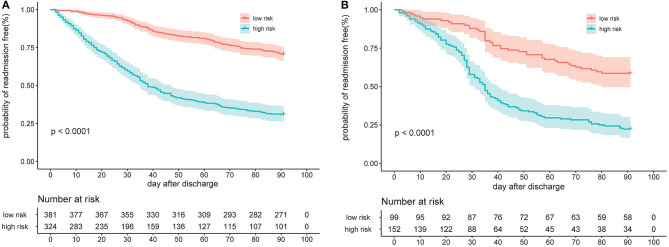
Background and Aims: Patients with acute decompensated (AD) cirrhosis are frequently readmitted to the hospital. An accurate predictive model for identifying high-risk patients may facilitate the development of effective interventions to reduce readmission rates. Methods: This cohort study of patients with AD cirrhosis was conducted at six tertiary hospitals in China between September 2012 and December 2016 (with 705 patients in the derivation cohort) and between January 2017 and April 2020 (with 251 patients in the temporal validation cohort). Least absolute shrinkage and selection operator Cox regression was used to identify the prognostic factors and construct a nomogram. The discriminative ability, calibration, and clinical net benefit were evaluated based on the C-index, area under the curve, calibration curve, and decision curve analysis. Kaplan-Meier curves were constructed for stratified risk groups, and log-rank tests were used to determine significant differences between the curves. Results: Among 956 patients, readmission rates were 24.58, 42.99, and 51.78%, at 30, 60, and 90 days, respectively. Bacterial infection was the main reason for index hospitalization and readmission. Independent factors in the nomogram included gastrointestinal bleeding [hazard rate (HR): 2.787; 95% confidence interval (CI): 2.221-3.499], serum sodium (HR: 0.955; 95% CI: 0.933-0.978), total bilirubin (HR: 1.004; 95% CI: 1.003-1.005), and international normalized ratio (HR: 1.398; 95% CI: 1.126-1.734). For the convenience of clinicians, we provided a web-based calculator tool (https://cqykdx1111.shinyapps.io/dynnomapp/). The nomogram exhibited good discrimination ability, both in the derivation and validation cohorts. The predicted and observed readmission probabilities were calibrated with reliable agreement. The nomogram demonstrated superior net benefits over other score models. The high-risk group (nomogram score >56.8) was significantly likely to have higher rates of readmission than the low-risk group (nomogram score ≤ 56.8; p < 0.0001). Conclusions: The nomogram is useful for assessing the probability of short-term readmission in patients with AD cirrhosis and to guide clinicians to develop individualized treatments based on risk stratification.
Keywords: acute decompensated cirrhosis; independent predictors; nomogram; readmission; risk stratification.
Copyright © 2021 Xu, Tan, Wang, Zhao and Qin.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
A New Scoring System for Predicting In-hospital Death in Patients Having Liver Cirrhosis With Esophageal Varices.Front Med (Lausanne). 2021 Oct 11;8:678646. doi: 10.3389/fmed.2021.678646. eCollection 2021. Front Med (Lausanne). 2021. PMID: 34708050 Free PMC article.
-
A Survival Prediction for Acute Heart Failure Patients via Web-Based Dynamic Nomogram with Internal Validation: A Prospective Cohort Study.J Inflamm Res. 2022 Mar 20;15:1953-1967. doi: 10.2147/JIR.S348139. eCollection 2022. J Inflamm Res. 2022. PMID: 35342297 Free PMC article.
-
An Externally Validated Dynamic Nomogram for Predicting Unfavorable Prognosis in Patients With Aneurysmal Subarachnoid Hemorrhage.Front Neurol. 2021 Aug 26;12:683051. doi: 10.3389/fneur.2021.683051. eCollection 2021. Front Neurol. 2021. PMID: 34512505 Free PMC article.
-
Development and external validation of a prognostic nomogram for acute decompensation of chronic hepatitis B cirrhosis.BMC Gastroenterol. 2018 Dec 3;18(1):179. doi: 10.1186/s12876-018-0911-y. BMC Gastroenterol. 2018. PMID: 30509201 Free PMC article.
-
Development and validation of a nomogram for esophagogastric variceal bleeding in liver cirrhosis: A cohort study in 1099 cases.J Dig Dis. 2022 Oct;23(10):597-609. doi: 10.1111/1751-2980.13145. J Dig Dis. 2022. PMID: 36400743 Review.
Cited by
-
Prospective multicentre randomised controlled trial to assess the clinical effectiveness of the novel CirrhoCare digital therapeutic management system: a study protocol.BMJ Open. 2025 Jul 6;15(7):e098725. doi: 10.1136/bmjopen-2024-098725. BMJ Open. 2025. PMID: 40623746 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous