

Coronary Arteries: Normal Anatomy With Historical Notes and Embryology of Main Stems
- PMID: 34136540
- PMCID: PMC8200569
- DOI: 10.3389/fcvm.2021.649855
Coronary Arteries: Normal Anatomy With Historical Notes and Embryology of Main Stems
Abstract
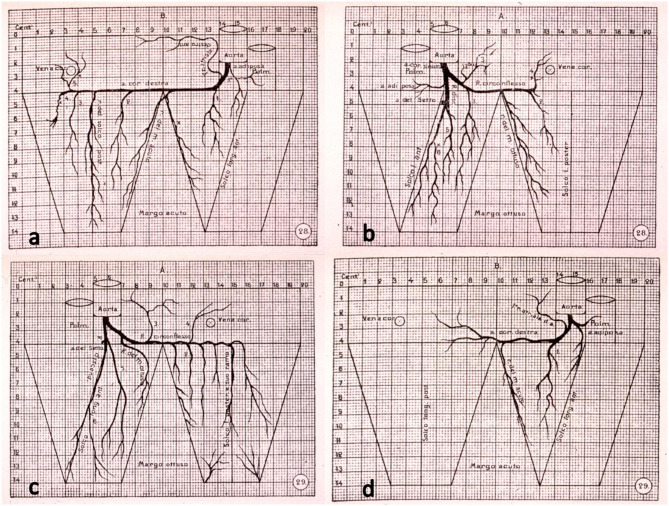
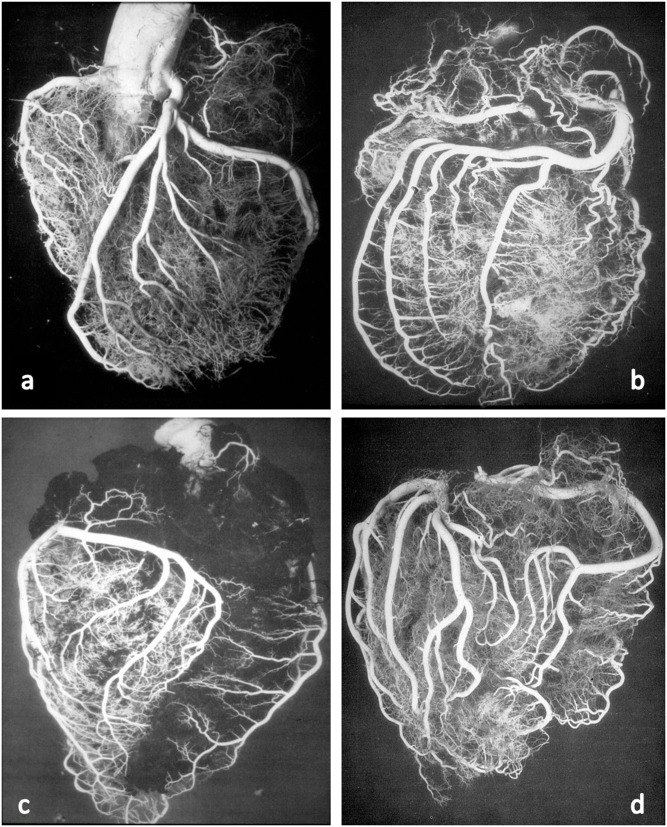
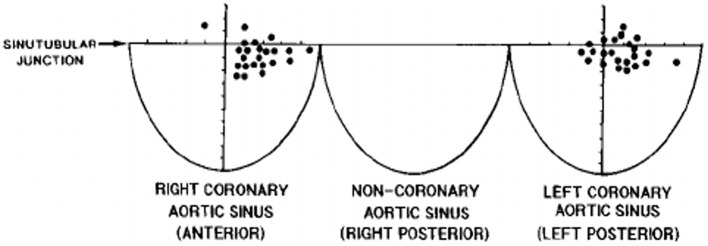
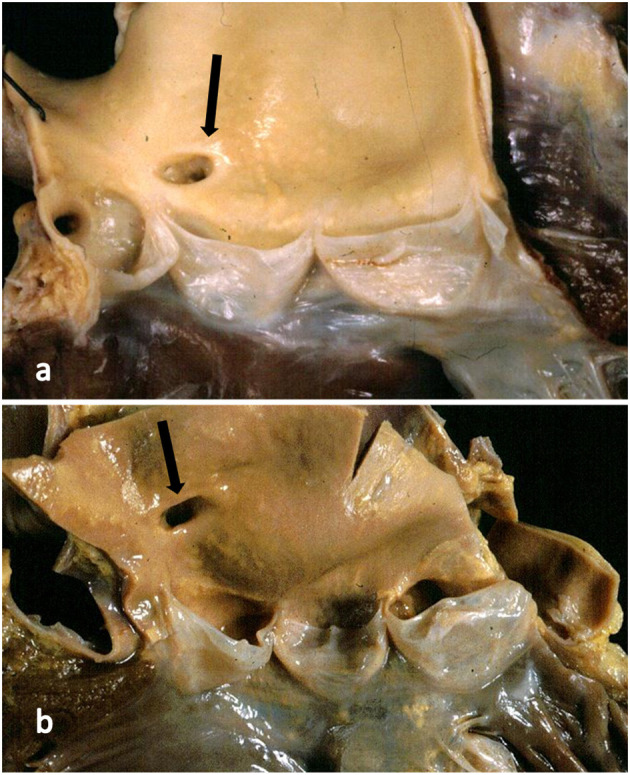
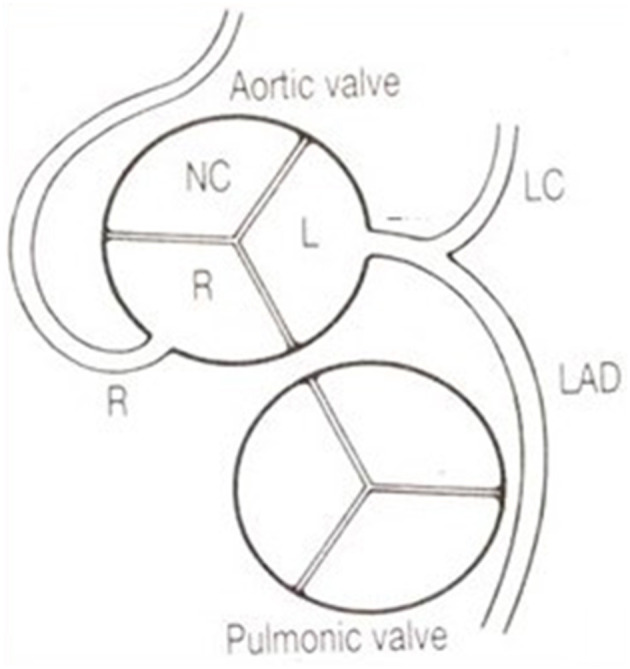
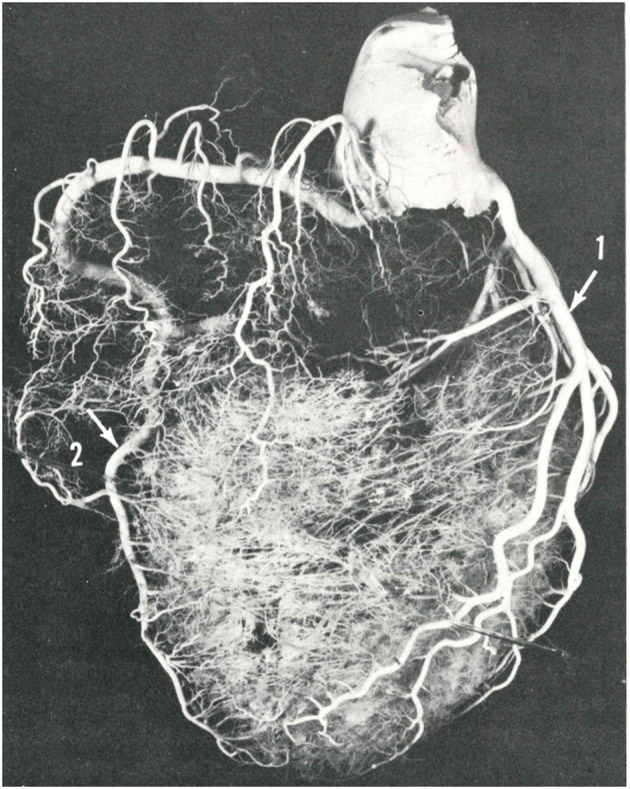
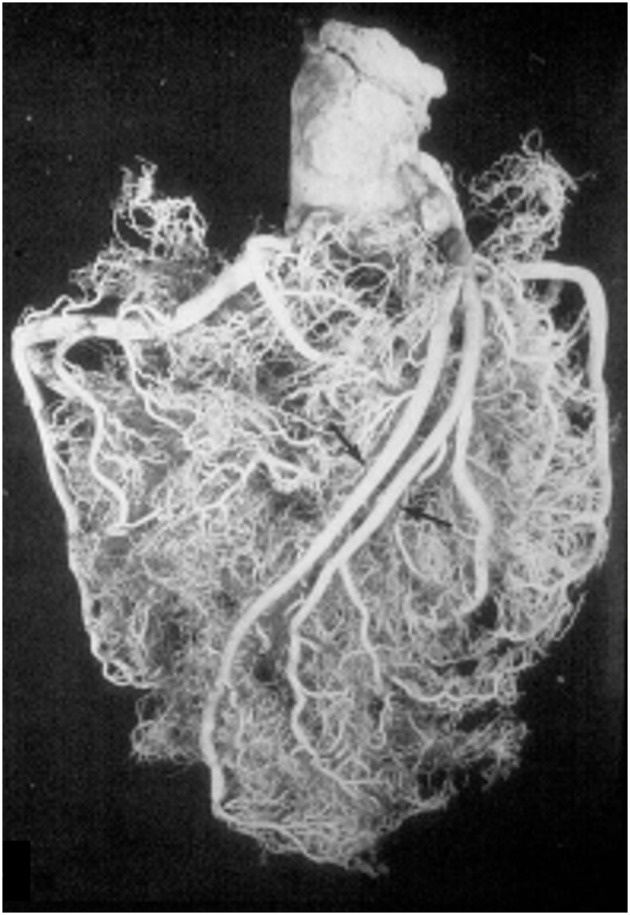
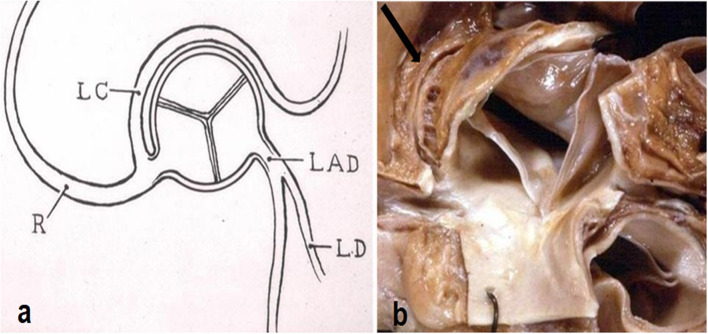
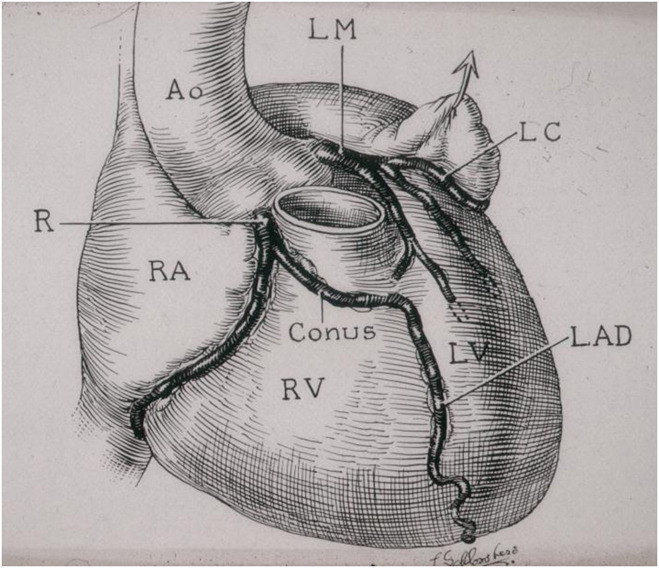
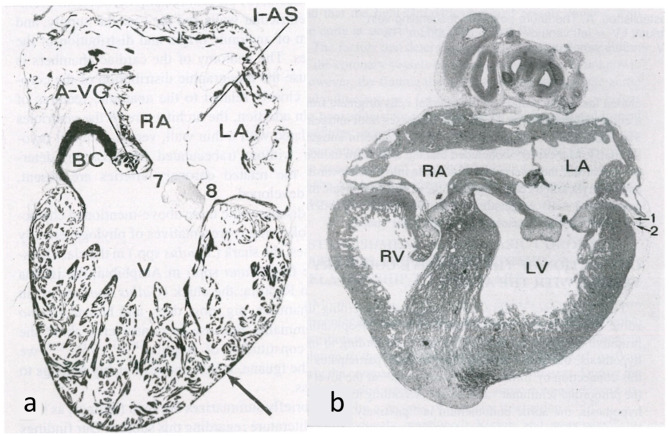
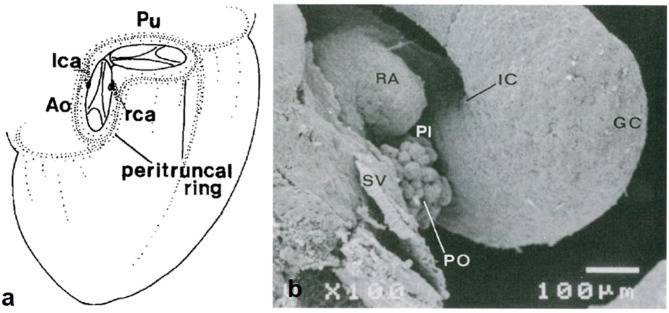
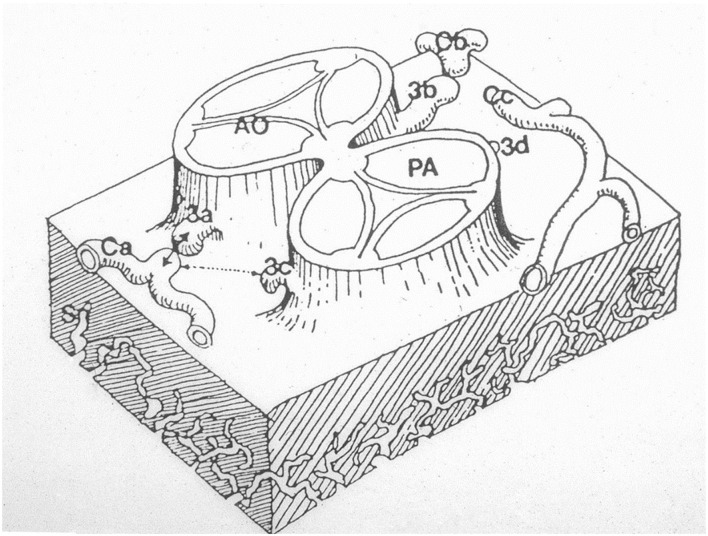
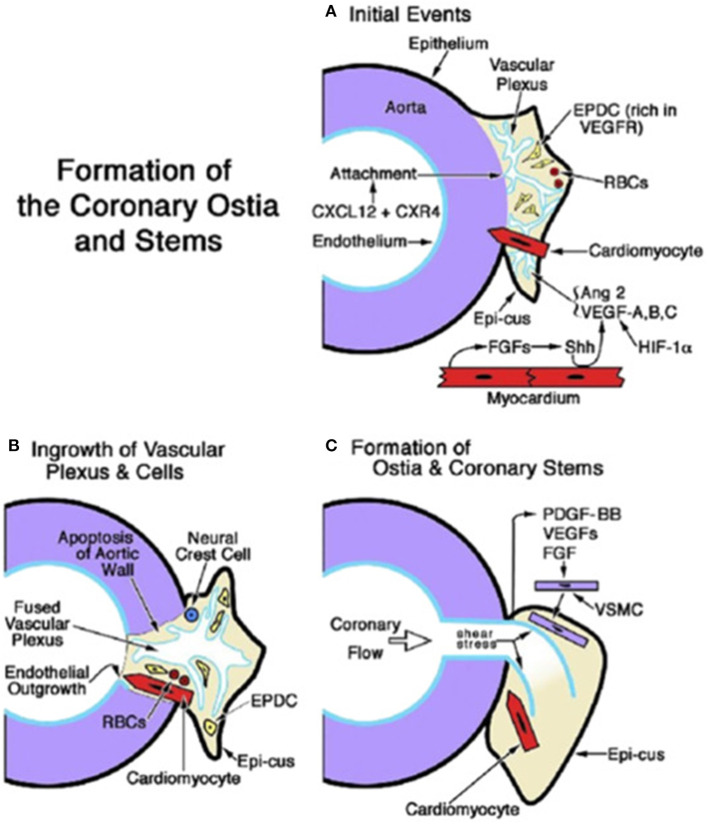
Anatomy of subepicardial coronary arteries became a topic of investigation at autopsy in Florence (Italy) by Banchi in the early twentieth century, with the discovery of dominant and balanced patterns. Thereafter, in the 60's of the same century Baroldi in Milan did post-mortem injection with spectacular three-dimensional casts. Later Sones at the Cleveland Clinic introduced selective coronary arteriography for in vivo visualization of coronary arteries. In the present chapter we show these patterns, as well as normal variants of origin and course with questionable risk of ischemia, like myocardial bridge as well as origin of the left circumflex coronary artery from the right sinus with retroaortic course. As far as embryology, the coronary arteries and veins are epicardial in origin and finally connect the former with the aorta, and the latter with the sinus venosus. At the time of spongy myocardium, intramural blood supply derives directly by the ventricular cavities, whereas later, at the time of myocardial compaction, vascularization originates from the subepicardial network. The connection of the subepicardial plexus with the aorta occurs with prongs of the peritruncal ring, which penetrate the facing aortic sinuses. Septation of truncus arteriosus is not responsible for the final position of the coronary orifices. Infact in transposition of the great arteries coronary ostia are regularly located within facing sinuses of the anterior aorta.
Keywords: anatomy; coronary arteries; embriology; history; normal variants.
Copyright © 2021 Thiene, Frescura, Padalino, Basso and Rizzo.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Morgagni GB. De Sedibus et Causis Morborum per a Anatomen Indagatis. Venice:Nabu Press (1761).
-
- Banchi A. Le variazioni delle arteriae coronariae cordis e la morfologia di questi vasi. Sperimentale. (1903) 57:367–69.
-
- Baroldi G, Scomazzoni G. Coronary Circulation in the Normal and Pathologic Heart. Washington DC: Office of the Surgeon General, Department of the Army (1967) p. 1–37.
-
- Sones FM, Shirey EK. Cine coronary arteriography. Mod Concepts Cardiovasc Dis. (1962) 31:735–8. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
Research Materials