

Osmotic Demyelination Syndrome: Clinical, Neuroimaging Characteristics, and Outcomes in a Series of 18 Cases
- PMID: 34136577
- PMCID: PMC8178002
- DOI: 10.1155/2021/9944632
Osmotic Demyelination Syndrome: Clinical, Neuroimaging Characteristics, and Outcomes in a Series of 18 Cases
Retraction in
-
Retracted: Osmotic Demyelination Syndrome: Clinical, Neuroimaging Characteristics, and Outcomes in a Series of 18 Cases.Biomed Res Int. 2024 Mar 20;2024:9847541. doi: 10.1155/2024/9847541. eCollection 2024. Biomed Res Int. 2024. PMID: 38550040 Free PMC article.
Abstract
Objective: To investigate the etiology, clinical as well as neuroimaging characteristics, and outcomes after proper treatment in a series of 18 patients with osmotic demyelination syndrome.
Methods: Medical records, including video records, of 18 patients with osmotic demyelination syndrome were retrospectively examined. Demographic and clinical information, imaging results, plans of management, and outcomes during the follow-up period were collected and analyzed.
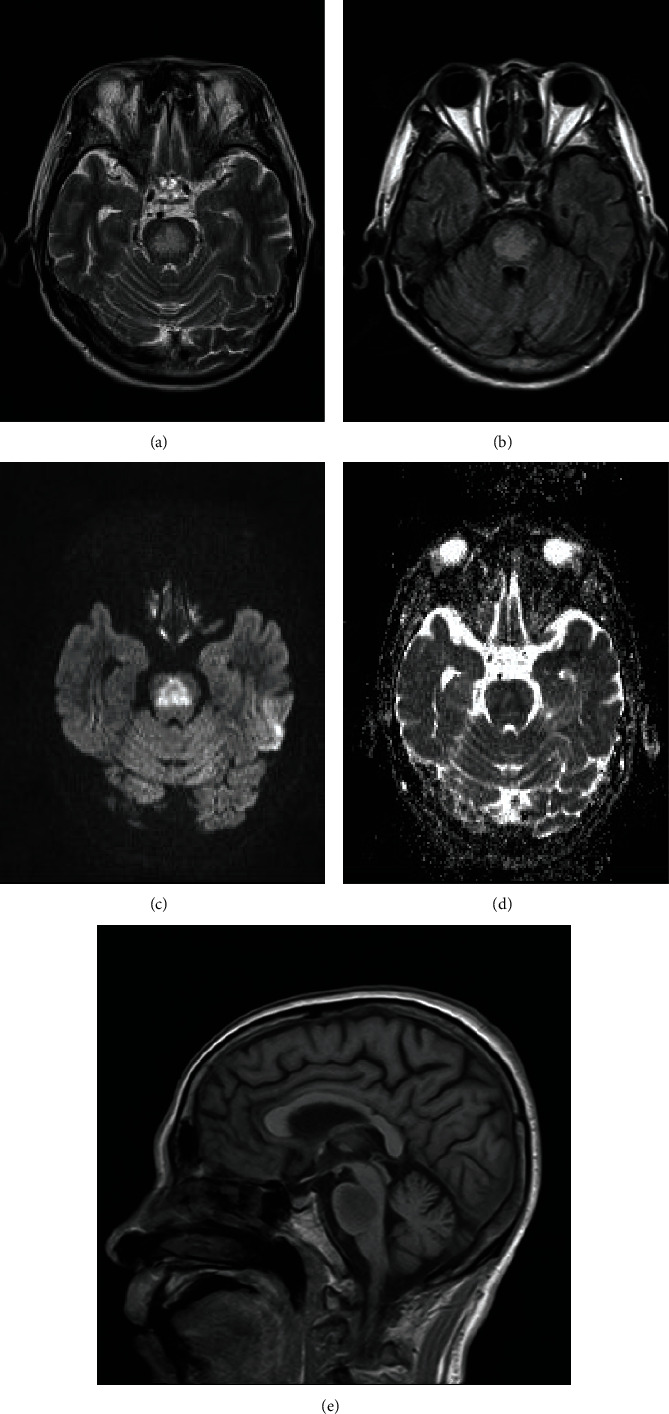
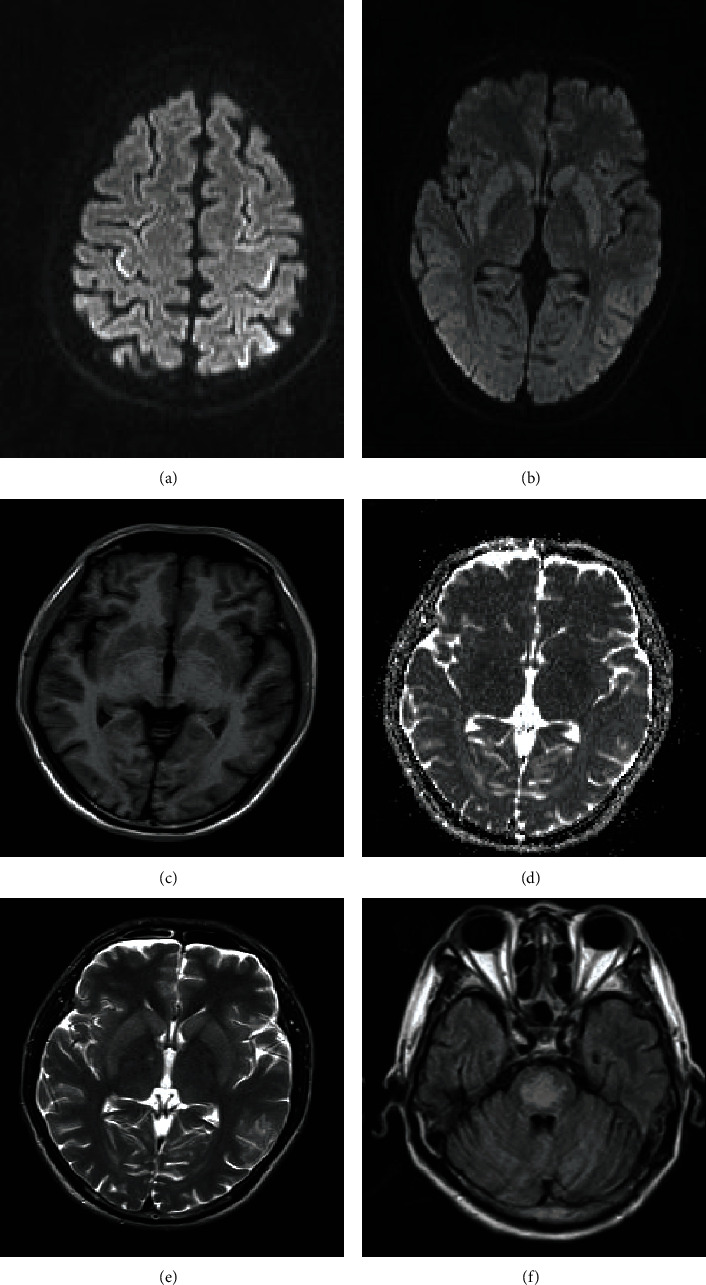
Results: Eighteen patients, including 10 males and 8 females, were included in the present study. The mean age at diagnosis of CNS insult was 47.4 ± 13.3 years (ranged from 30 to 78 years). Etiologies included rapidly corrected hyponatremia (50%), alcoholism (27.8%), and others. Neurological manifestations included encephalopathy (61.1%), dysphonia (50%), extrapyramidal symptoms (38.9%), and seizures (22.2%). Neuroimaging results showed that 6 patients (33.3%) had central pontine myelinolysis, 5 (27.8%) had extrapontine myelinolysis, and 7 (38.9%) had both. After treatment, 12 patients showed improvement and the other 6 did not. Among these patients, those who showed symptoms of encephalopathy had a favorable outcome. The majority of those who presented with mental retardation, seizures, and no other symptoms recovered better than their counterparts who had other symptoms. Nine out of 11 patients with pseudobulbar paralysis and/or extrapyramidal symptoms showed improvement, but the other 2 did not show improvement. Five patients who did not improve after treatment during admission were followed up for 1-3 months with rehabilitation training recommended, and it was found that 3 showed significant improvement after training, and the other 2 did not respond to this training.
Conclusions: Osmotic demyelination syndrome is a complex disease entity due to a variety of etiologies, manifesting with symptoms involving diverse systems of the brain. Early identification and removal/correction of conditions leading to osmotic demyelination syndrome are the key to prevent and/or manage this disease.
Copyright © 2021 Xinhuang Lv et al.
Conflict of interest statement
The authors declare that there is no conflict of interests.
Figures
References
-
- Kallakatta R. N., Radhakrishnan A., Fayaz R. K., Unnikrishnan J. P., Kesavadas C., Sarma S. P. Clinical and functional outcome and factors predicting prognosis in osmotic demyelination syndrome (central pontine and/or extrapontine myelinolysis) in 25 patients. Journal of Neurology Neurosurgery and Psychiatry. 2011;82(3):326–331. doi: 10.1136/jnnp.2009.201764. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
