

Short-term reoperation risk after surgical and nonsurgical management of isolated greater tuberosity fractures
- PMID: 34136866
- PMCID: PMC8178603
- DOI: 10.1016/j.jseint.2020.12.002
Short-term reoperation risk after surgical and nonsurgical management of isolated greater tuberosity fractures
Abstract
Background: The outcomes and complication rates of patients with isolated greater tuberosity fractures are not well documented. The present study aimed to evaluate the reoperation rates, types of reoperations, and complications for patients undergoing open reduction internal fixation and those undergoing initial nonoperative treatment of isolated greater tuberosity fractures.
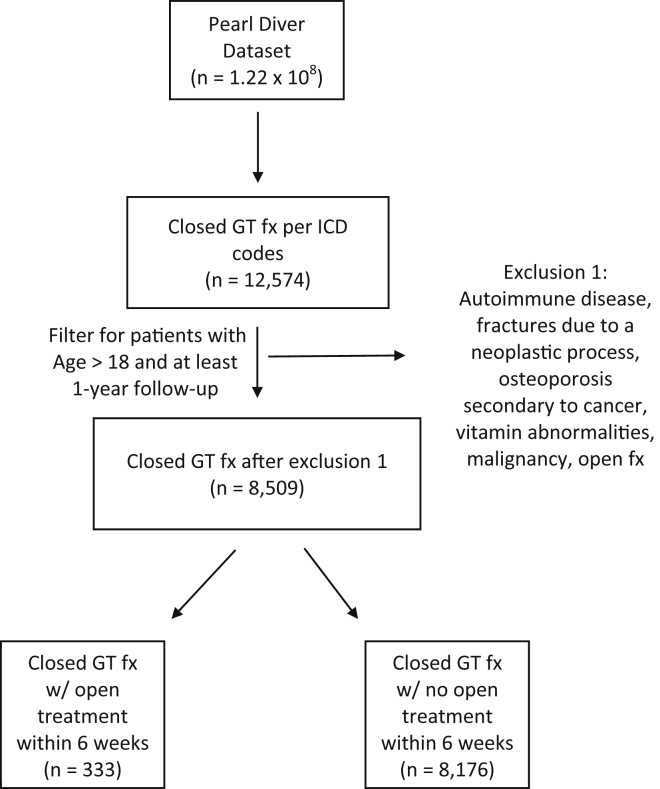
Methods: An administrative claims database was queried from 2010 to 2018 for adult patients treated with open reduction internal fixation or initial nonoperative treatment within 6 weeks of sustaining a closed isolated greater tuberosity fracture. Reoperation rates, types of reoperations, local/surgical complications, and systemic complications for two cohorts were collected, and statistical analysis was performed using R statistical software for patients initially treated operatively and nonoperatively. Complication rates were compared using multivariate logistic regression, while demographic data were compared using chi-square analysis.
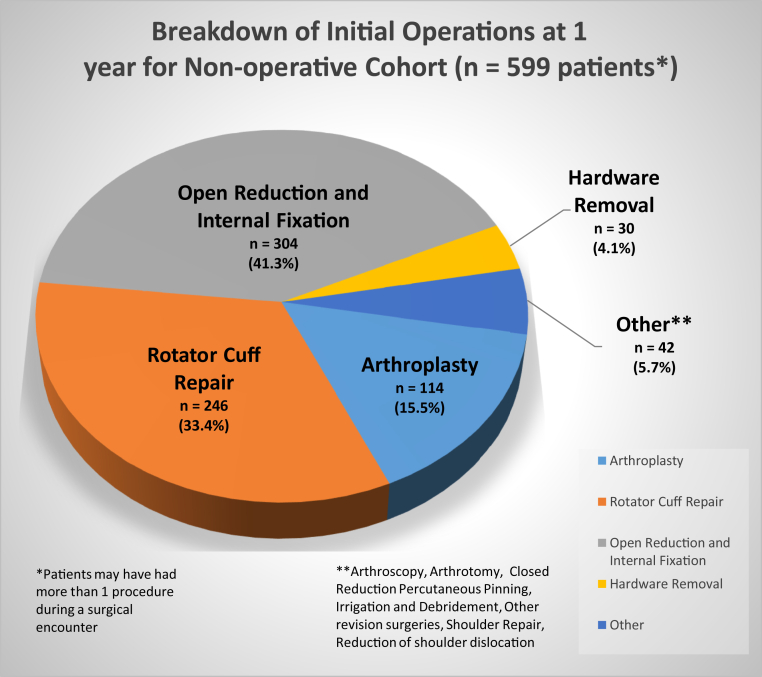
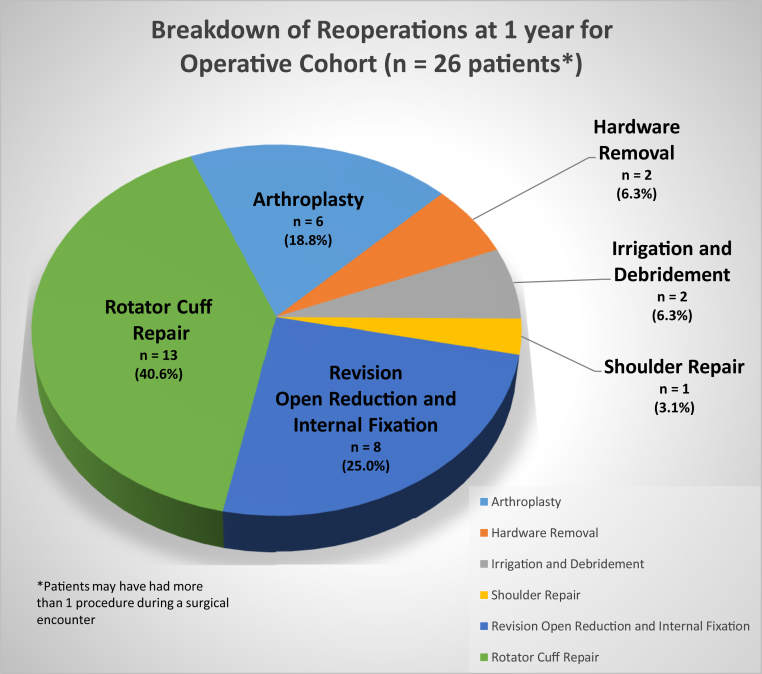
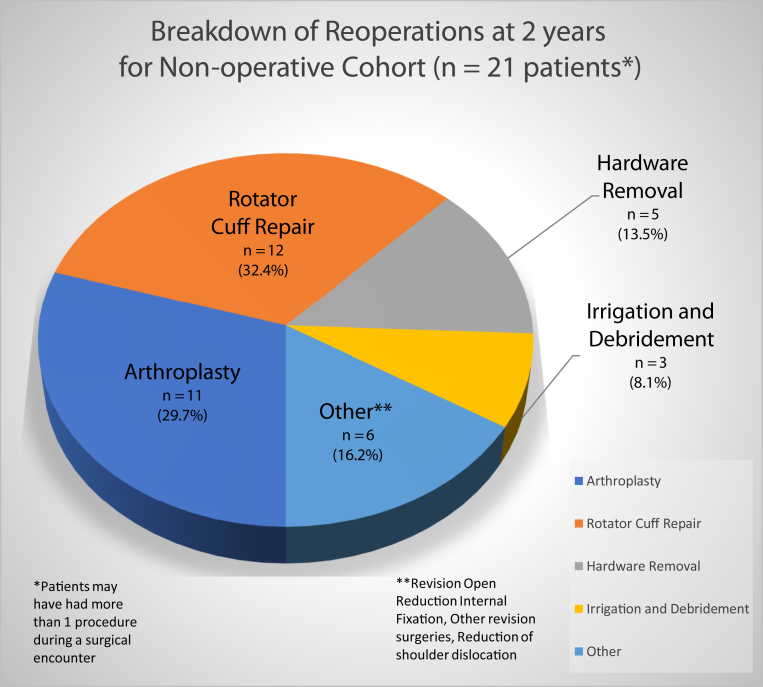
Results: Of the 8509 patients who were documented to have sustained a closed isolated greater tuberosity fracture, 333 patients underwent operative treatment and 8176 patients received initial nonoperative treatment within the first 6 weeks of diagnosis. The operative cohort had a reoperation rate of 2.7% at 90 days, 5.7% at 6 months, and 7.8% at 1 year, with the majority of reoperations being rotator cuff repair (40.6%). Within the initial nonoperative cohort, 7.3% had an operation within a year, with the majority of operations being open reduction internal fixation (41.3%). The subsequent reoperation rate for those patients was 3.5% at 2 years with the majority of reoperations being rotator cuff repair (32.4%). In the operative cohort, the 90-day infection rate was 3.0%. Nonunion was demonstrated in the operative cohort at a rate of 1.8% at 6 months and 2.7% at 1 year.
Conclusion: When surgical care was provided to patients sustaining isolated greater tuberosity fractures in the first 6 weeks, there was a 7.8% rate of reoperation within the first year. Patients initially treated nonoperatively had a future operation rate of 7.3% within the first year and a 3.5% reoperation rate within the second year. The most common reoperation regardless of initial treatment was rotator cuff repair. With an elevated rate of subsequent operations, education is paramount to provide patients with expectations for the sequelae of this injury especially when presenting with concomitant injuries.
Keywords: Isolated greater tuberosity fracture; Local complications; Nonoperative treatment; Operative treatment; Reoperation rates; Reoperation types; Systemic complications.
© 2021 The Author(s).
Figures
References
-
- Barlow J.D. Complications after ORIF of proximal humerus fractures—how to deal with them. Ann Jt. 2020 doi: 10.21037/aoj-20-77. - DOI
-
- Bhatia D.N., van Rooyen K.S., du Toit D.F., de Beer J.F. Surgical treatment of comminuted, displaced fractures of the greater tuberosity of the proximal humerus: a new technique of double-row suture-anchor fixation and long-term results. Injury. 2006;37:946–952. doi: 10.1016/j.injury.2006.06.009. - DOI - PubMed
LinkOut - more resources
Full Text Sources