

Results of standardized treatment of elbow fracture dislocations as per their injury pattern: a retrospective cohort of 89 patients
- PMID: 34136875
- PMCID: PMC8178606
- DOI: 10.1016/j.jseint.2020.12.004
Results of standardized treatment of elbow fracture dislocations as per their injury pattern: a retrospective cohort of 89 patients
Abstract
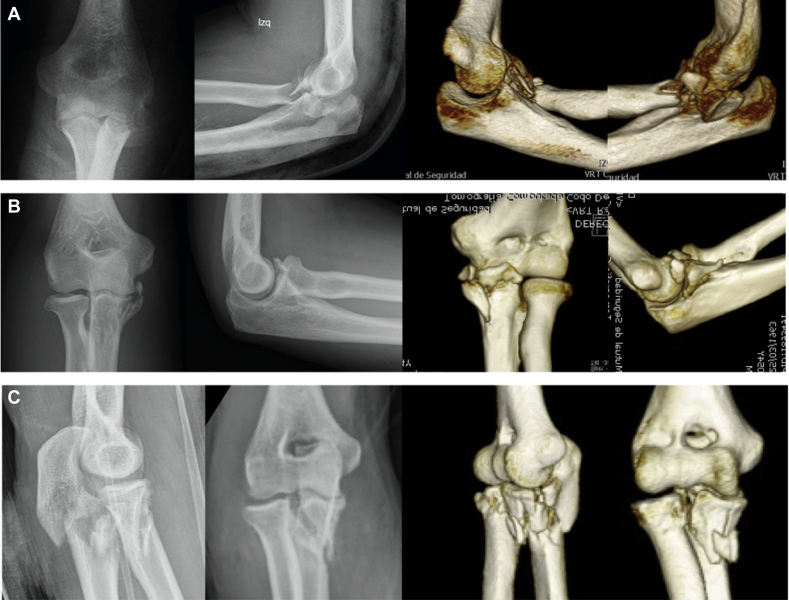
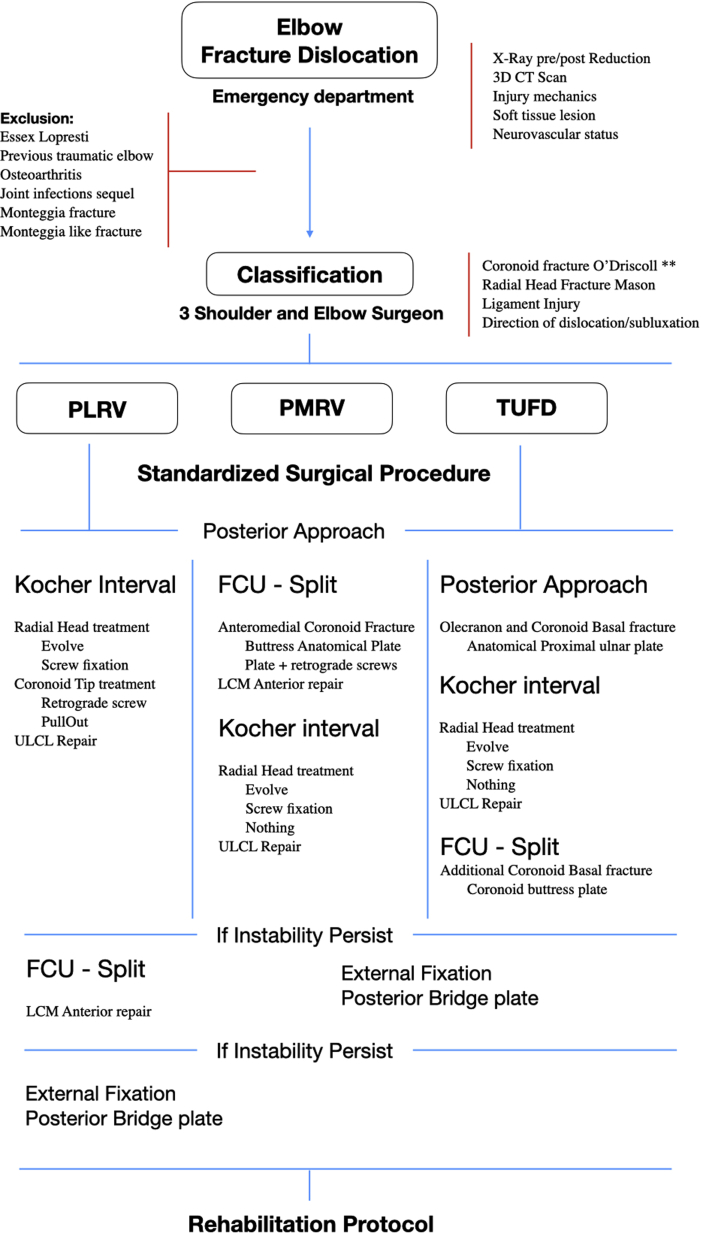
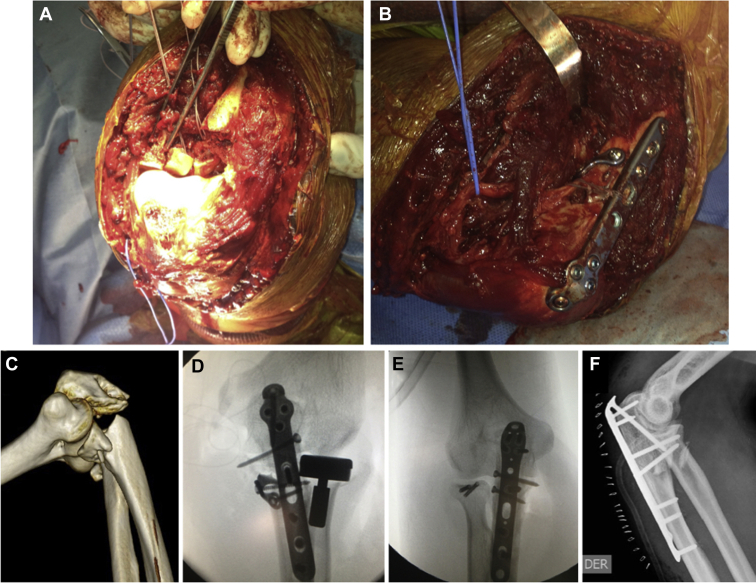
Background: Elbow fracture dislocations represent difficult injuries to treat, with a high percentage of complications. Classically, they are divided into posterolateral, posteromedial and transulnar pattern. It is essential to distinguish them to guide intraoperative treatment to achieve an anatomic and stable reduction that allows early mobility.
Methods: A retrospective study of 89 adult patients diagnosed with elbow fracture dislocations who underwent a standardized surgery between 2013 and 2018 with a minimum follow-up of 12 months. Demographic data, characteristics of the injury, and associated procedures were collected. Patients were evaluated with functional scores (Mayo elbow performance score/Broberg and Morrey score) and ranges of movement at the end of the follow-up.
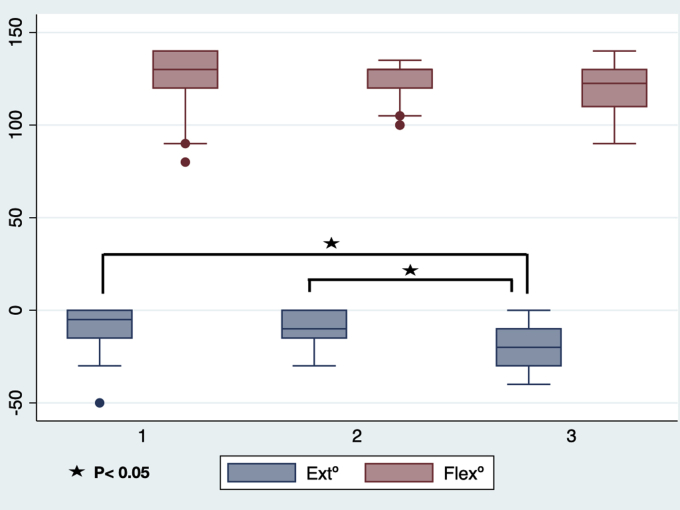
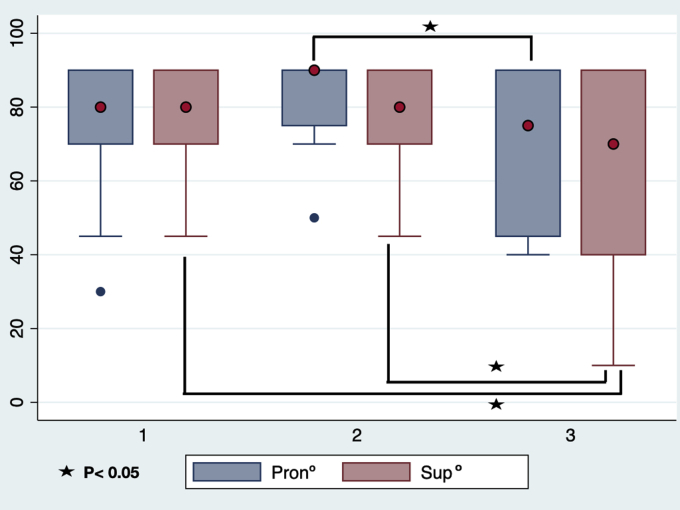
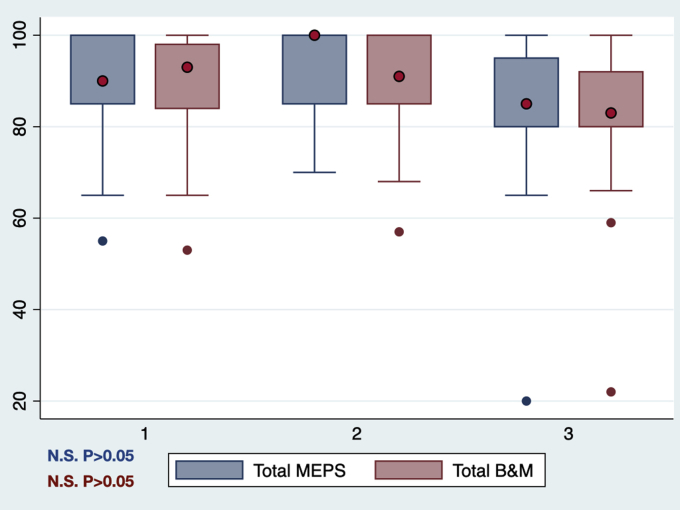
Results: The mean age was 41 ± 12 years, mostly men (82%), with an average follow-up of 29 months. We present 42 patients with posterolateral fracture dislocation (47%), 21 posteromedial (24%) and 26 transulnar (29%). The average range of motion at the end of follow-up was -12 ± 11° extension, 124 ± 20° flexion, 76 ± 16° pronation, and 73 ± 20° supination, with a Mayo elbow performance score of 88.7 ± 12 points and 87.2 ± 12 points in the Broberg and Morrey scale. Reoperation rate was 23%, with no infection or heterotopic ossification cases. Transulnar fracture dislocations have significantly worse extension and supination. As per the functional result (Mayo elbow performance score/Broberg and Morrey scale), there are no significant differences between the different patterns.
Conclusion: Proper injury pattern recognition and a standardized surgical management lead to a stable joint and good results in range of motion. Functional results are encouraging at least at short term, despite the high reoperations rate.
Keywords: Clinical outcomes; Coronoid fracture; Elbow fracture dislocations; Elbow instability; Elbow terrible triad; Transulnar fracture; Workers compensation.
© 2021 The Authors.
Figures
Similar articles
-
Transolecranon fracture dislocation and transolecranon basal coronoid fracture dislocation; results of standardized treatment in a retrospective cohort.JSES Int. 2024 Dec 13;9(3):878-884. doi: 10.1016/j.jseint.2024.11.019. eCollection 2025 May. JSES Int. 2024. PMID: 40486785 Free PMC article.
-
Lasso plate - An original implant for fixation of type I and II Regan-Morrey coronoid fractures.Orthop Traumatol Surg Res. 2017 May;103(3):447-451. doi: 10.1016/j.otsr.2016.12.017. Epub 2017 Feb 7. Orthop Traumatol Surg Res. 2017. PMID: 28185992
-
[Extensor digitorum communis split approach combined with loop-plate technique for treatment of ulnar coronoid fracture in terrible triad of elbow].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2021 Apr 15;35(4):420-425. doi: 10.7507/1002-1892.202010081. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2021. PMID: 33855824 Free PMC article. Chinese.
-
Trans-Olecranon Fracture-Dislocations of the Elbow: A Systematic Review.Diagnostics (Basel). 2020 Dec 6;10(12):1058. doi: 10.3390/diagnostics10121058. Diagnostics (Basel). 2020. PMID: 33291269 Free PMC article. Review.
-
Treatment of complex elbow fracture-dislocations.Curr Rev Musculoskelet Med. 2016 Jun;9(2):185-9. doi: 10.1007/s12178-016-9337-8. Curr Rev Musculoskelet Med. 2016. PMID: 26984334 Free PMC article. Review.
Cited by
-
Differences in outcome and complications between 2 distinct complex traumatic elbow instability patterns. A retrospective comparison of terrible triad and olecranon fracture dislocations.JSES Int. 2025 Feb 15;9(3):912-919. doi: 10.1016/j.jseint.2025.01.019. eCollection 2025 May. JSES Int. 2025. PMID: 40486766 Free PMC article.
-
Characteristics of rehabilitation protocols following operative treatment of terrible triad elbow injuries and the influence of early motion: A systematic review and meta-analysis.Shoulder Elbow. 2024 Aug 6:17585732241269807. doi: 10.1177/17585732241269807. Online ahead of print. Shoulder Elbow. 2024. PMID: 39552691 Free PMC article. Review.
-
Transolecranon fracture dislocation and transolecranon basal coronoid fracture dislocation; results of standardized treatment in a retrospective cohort.JSES Int. 2024 Dec 13;9(3):878-884. doi: 10.1016/j.jseint.2024.11.019. eCollection 2025 May. JSES Int. 2024. PMID: 40486785 Free PMC article.
-
Radial head arthroplasty vs. open reduction and internal fixation for the treatment of terrible triad injury of the elbow: A systematic review and meta-analysis update.Exp Ther Med. 2022 Jul 27;24(3):592. doi: 10.3892/etm.2022.11529. eCollection 2022 Sep. Exp Ther Med. 2022. PMID: 35949335 Free PMC article.
-
Surgical management of elbow heterotopic ossification: postoperative outcomes with and without continuous passive motion rehabilitation.JSES Int. 2025 Mar 5;9(3):924-928. doi: 10.1016/j.jseint.2025.02.002. eCollection 2025 May. JSES Int. 2025. PMID: 40486814 Free PMC article.
References
-
- Broberg M.A., Morrey B.F. Results of treatment of fracture-dislocations of the elbow. Clin Orthop. 1987;216:109–119. - PubMed
-
- Celi A. Anatomy and biomechanics of the elbow. In: Celli A., Morrey L., Morrey B.F., editors. Treatment of Elbow Lesions, New Aspects in Diagnosis and Surgical Techniques. 1st ed. Springer-Verlag Mailand; Milán: 2008. pp. 12–22.
LinkOut - more resources
Full Text Sources
Research Materials