

Diagnosis of wild-type transthyretin amyloid cardiomyopathy in Japan: red-flag symptom clusters and diagnostic algorithm
- PMID: 34137515
- PMCID: PMC8318452
- DOI: 10.1002/ehf2.13473
Diagnosis of wild-type transthyretin amyloid cardiomyopathy in Japan: red-flag symptom clusters and diagnostic algorithm
Abstract
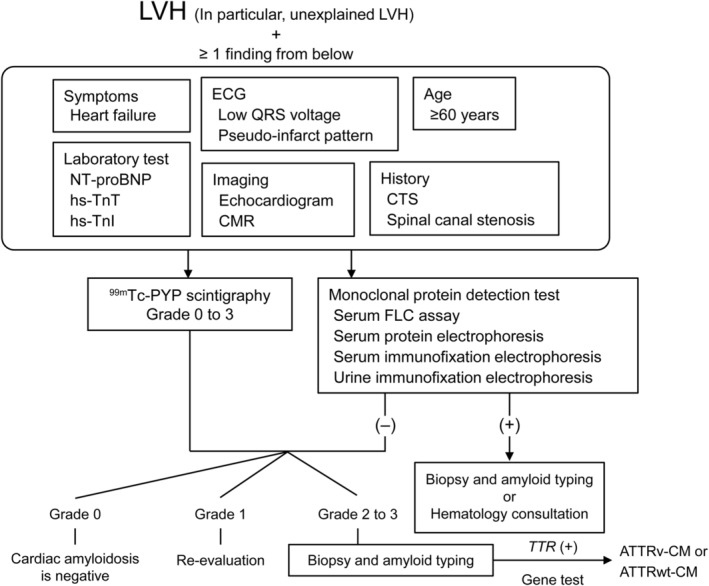
Wild-type transthyretin amyloid cardiomyopathy (ATTRwt-CM) is caused by the deposition of wild-type transthyretin (TTR) amyloid fibrils in the heart. The age at diagnosis of ATTRwt-CM is reported to be approximately 70-80 years, and patients commonly present with non-disease-specific cardiac abnormalities, such as heart failure with preserved ejection fraction and diastolic dysfunction. The disease can be fatal if left untreated, with an approximate survival of 3-5 years from diagnosis. An oral TTR stabilizer, tafamidis, has enabled early intervention for the treatment of ATTRwt-CM. However, awareness of ATTRwt-CM remains low, and misdiagnosis and a delay in diagnosis are common. This review discusses the epidemiology, characteristics, treatment strategy, and red-flag symptoms and signs of ATTRwt-CM based on the published literature, as well as recent advances in diagnostic modalities that enable early and accurate diagnosis of the disease. We also discuss an algorithm for early and accurate diagnosis of ATTRwt-CM in daily clinical practice. In our diagnostic algorithm, a suspected diagnosis of ATTRwt-CM should be triggered by unexplained left ventricular hypertrophy (LVH), which is LVH that cannot be explained by an increased afterload due to hypertension or valvular disease. In addition, heart failure symptoms, laboratory test results (N-terminal pro-B-type natriuretic peptide, high-sensitivity troponin T, or high-sensitivity troponin I), electrocardiogram and imaging (echocardiogram or cardiac magnetic resonance) data, age (≥60 years), and medical history suggestive of ATTRwt-CM (e.g. carpal tunnel syndrome) should be examined. Detailed examinations using bone scintigraphy and monoclonal protein detection tests followed by tissue biopsy, amyloid typing, and TTR genetic testing are warranted for a definite diagnosis of ATTRwt-CM.
Keywords: ATTRwt-CM; Biopsy; Carpal tunnel syndrome; HFpEF; Scintigraphy; Tafamidis.
© 2021 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
Takayuki Inomata has received consulting fees or honoraria from Daiichi‐Sankyo Co., Japan Medtronics Co., Mitsubishi Tanabe Pharma Co., Otsuka Pharmaceutical Co., Pfizer Inc., Bristol‐Myers Squibb, and Boehringer Ingelheim GmbH. M.U. has received consulting fees or honoraria, support for travel to meetings, and administrative support for writing assistance, medicines, or equipment from Pfizer Inc. for the submitted work and reports financial relationships outside of the submitted work with Pfizer Inc. and Alnylam Pharmaceuticals Inc. Tomonori Ishii and Y.K. are full‐time employees of Pfizer Pharmaceuticals K.K. J.K. has received consulting fees or honoraria and support for travel to meetings from Pfizer Inc. N.T., K.N., and J.E. report no conflicts of interest.
Figures
References
-
- Falk RH, Comenzo RL, Skinner M. The systemic amyloidoses. N Engl J Med 1997; 337: 898–909. - PubMed
-
- Kitaoka H, Izumi C, Izumiya Y, Inomata T, Ueda M, Kubo T, Koyama J, Sano M, Sekijima Y, Tahara N, Tsukada N, Tsujita K, Tsutsui H, Tomita T, Amano M, Endo J, Okada A, Oda S, Takashio S, Baba Y, Misumi Y, Yazaki M, Anzai T, Ando Y, Isobe M, Kimura T, Fukuda K, Japanese Circulation Society Joint Working Group . JCS 2020 guideline on diagnosis and treatment of cardiac amyloidosis. Circ J 2020; 84: 1610–1671. - PubMed
-
- Gillmore JD, Maurer MS, Falk RH, Merlini G, Damy T, Dispenzieri A, Wechalekar AD, Berk JL, Quarta CC, Grogan M, Lachmann HJ, Bokhari S, Castano A, Dorbala S, Johnson GB, Glaudemans AW, Rezk T, Fontana M, Palladini G, Milani P, Guidalotti PL, Flatman K, Lane T, Vonberg FW, Whelan CJ, Moon JC, Ruberg FL, Miller EJ, Hutt DF, Hazenberg BP, Rapezzi C, Hawkins PNS. Nonbiopsy diagnosis of cardiac transthyretin amyloidosis. Circulation 2016; 133: 2404–2412. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
