

Practice, Outcomes, and Complications of Emergent Endotracheal Intubation by Critical Care Practitioners During the COVID-19 Pandemic
- PMID: 34139207
- PMCID: PMC8204844
- DOI: 10.1016/j.chest.2021.06.008
Practice, Outcomes, and Complications of Emergent Endotracheal Intubation by Critical Care Practitioners During the COVID-19 Pandemic
Abstract
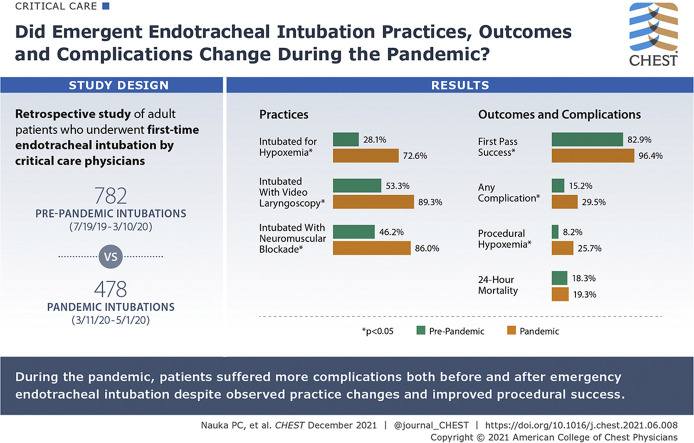
Background: For patients with COVID-19 who undergo emergency endotracheal intubation, data are limited regarding the practice, outcomes, and complications of this procedure.
Research question: For patients with COVID-19 requiring emergency endotracheal intubation, how do the procedural techniques, the incidence of first-pass success, and the complications associated with the procedure compare with intubations of critically ill patients before the COVID-19 pandemic?
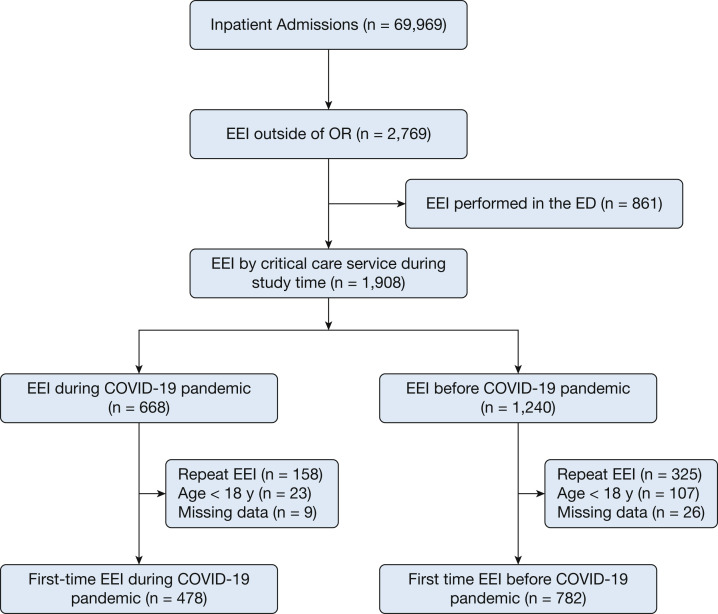
Study design and methods: We conducted a retrospective study of adult patients with COVID-19 at Montefiore Medical Center who underwent first-time endotracheal intubation by critical care physicians between July 19, 2019, and May 1, 2020. The first COVID-19 patient was admitted to our institution on March 11, 2020; patients admitted before this date are designated the prepandemic cohort. Descriptive statistics were used to compare groups. A Fisher exact test was used to compare categorical variables. For continuous variables, a two-tailed Student t test was used for parametric variables or a Wilcoxon rank-sum test was used for nonparametric variables.
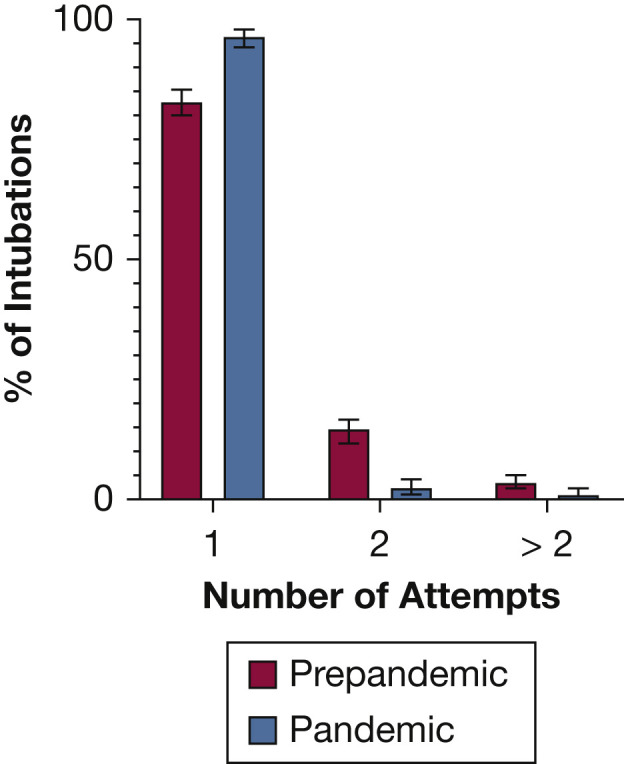
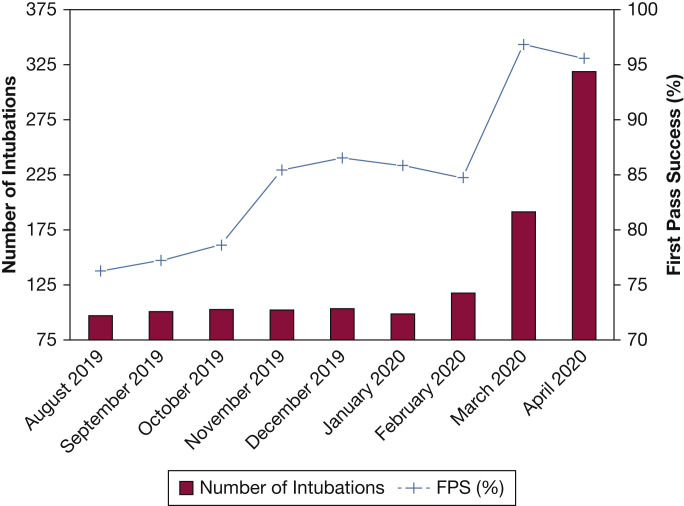
Results: One thousand two hundred sixty intubations met inclusion criteria (782 prepandemic cohort, 478 pandemic cohort). Patients during the pandemic were more likely to be intubated for hypoxemic respiratory failure (72.6% vs 28.1%; P < .01). During the pandemic, operators were more likely to use video laryngoscopy (89.4% vs 53.3%; P < .01) and neuromuscular blocking agents (86.0% vs 46.2%; P < .01). First-pass success was higher during the pandemic period (94.6% vs 82.9%; P < .01). The rate of associated complications was higher during the pandemic (29.5% vs 15.2%; P < .01), a finding driven by a higher rate of hypoxemia during or immediately after the procedure (25.7% vs 8.2%; P < .01).
Interpretation: Video laryngoscopy and neuromuscular blockade were used increasingly during the COVID-19 pandemic. Despite a higher rate of first-pass success during the pandemic, the incidence of complications associated with the procedure was higher.
Keywords: airway management; intratracheal; intubation; mechanical ventilation.
Copyright © 2021. Published by Elsevier Inc.
Figures
Comment in
-
Evolving Tracheal Intubation Practice Patterns in the Pandemic Era.Chest. 2021 Dec;160(6):1993-1994. doi: 10.1016/j.chest.2021.07.002. Chest. 2021. PMID: 34872660 Free PMC article. No abstract available.
References
-
- Chand S., Kapoor S., Orsi D., et al. COVID-19-associated critical illness-report of the first 300 patients admitted to intensive care units at a New York City medical center. J Intensive Care Med. 2020;35(10):963–970. - PubMed
-
- Cook T.M., El-Boghdadly K., McGuire B., McNarry A.F., Patel A., Higgs A. Consensus guidelines for managing the airway in patients with COVID-19: guidelines from the Difficult Airway Society, the Association of Anaesthetists the Intensive Care Society, the Faculty of Intensive Care Medicine and the Royal College of Anaesthetists. Anaesthesia. 2020;75(6):785–799. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
