

Triglycerides and Residual Atherosclerotic Risk
- PMID: 34140107
- PMCID: PMC8215641
- DOI: 10.1016/j.jacc.2021.04.059
Triglycerides and Residual Atherosclerotic Risk
Abstract
Background: Even when low-density lipoprotein-cholesterol (LDL-C) levels are lower than guideline thresholds, a residual risk of atherosclerosis remains. It is unknown whether triglyceride (TG) levels are associated with subclinical atherosclerosis and vascular inflammation regardless of LDL-C.
Objectives: This study sought to assess the association between serum TG levels and early atherosclerosis and vascular inflammation in apparently healthy individuals.
Methods: An observational, longitudinal, and prospective cohort study, including 3,754 middle-aged individuals with low to moderate cardiovascular risk from the PESA (Progression of Early Subclinical Atherosclerosis) study who were consecutively recruited between June 2010 and February 2014, was conducted. Peripheral atherosclerotic plaques were assessed by 2-dimensional vascular ultrasound, and coronary artery calcification (CAC) was assessed by noncontrast computed tomography, whereas vascular inflammation was assessed by fluorine-18 fluorodeoxyglucose uptake on positron emission tomography.
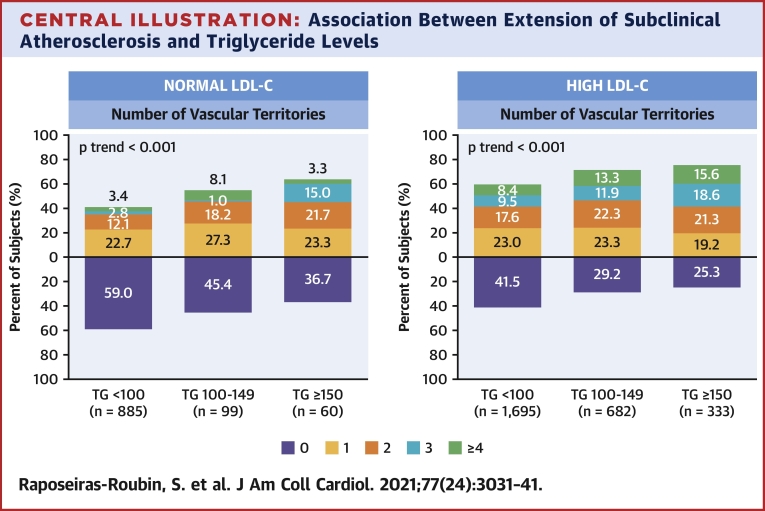
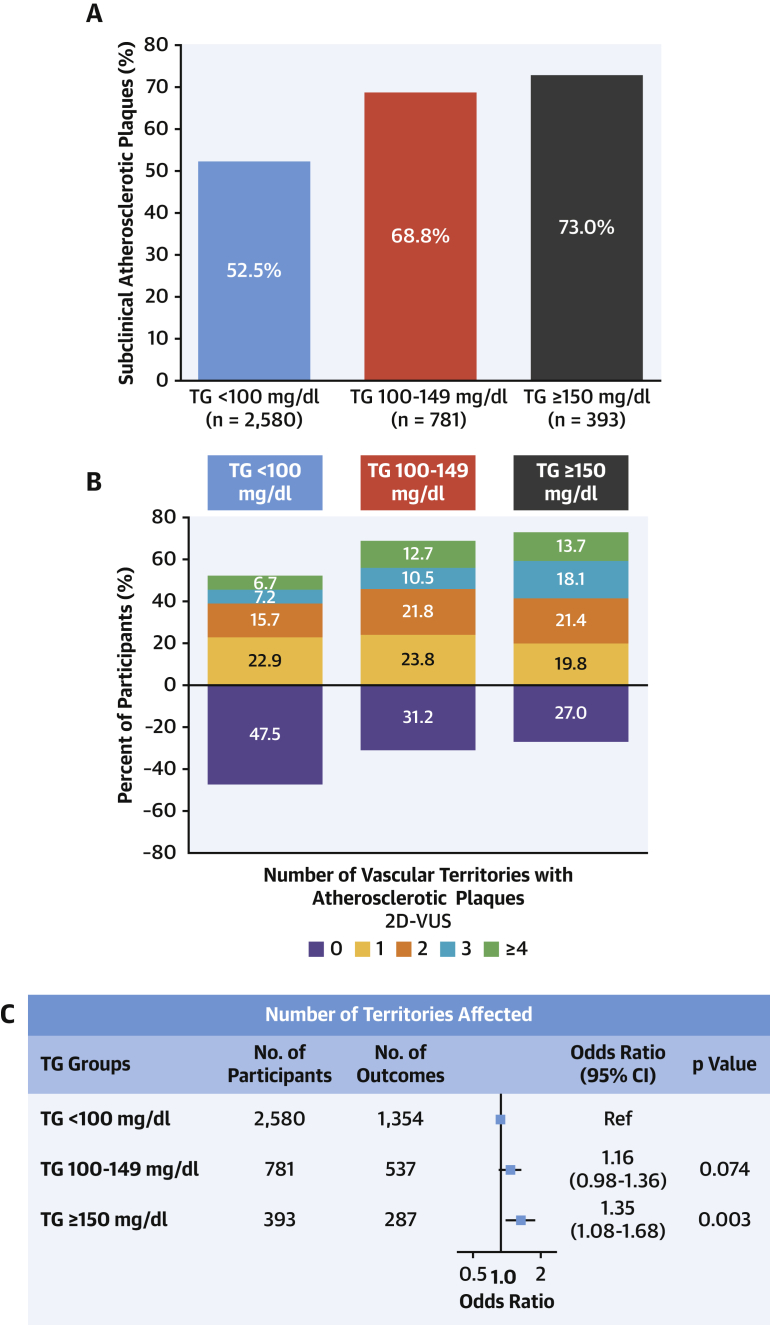
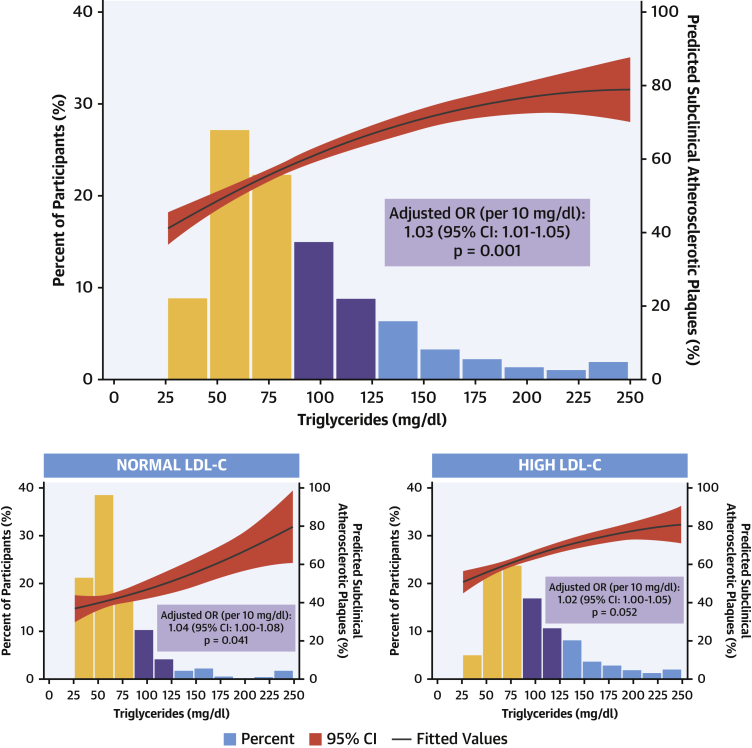
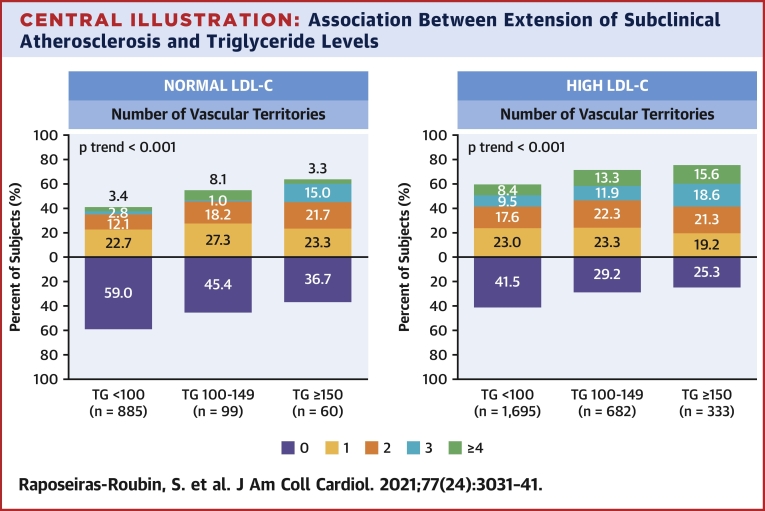
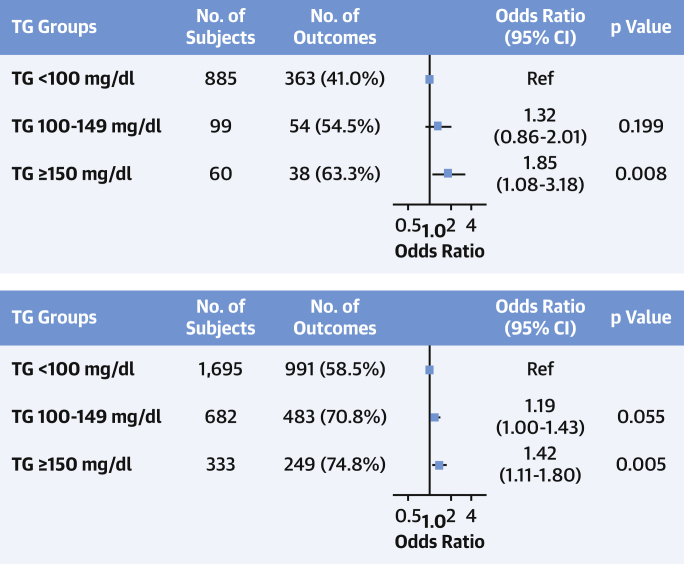
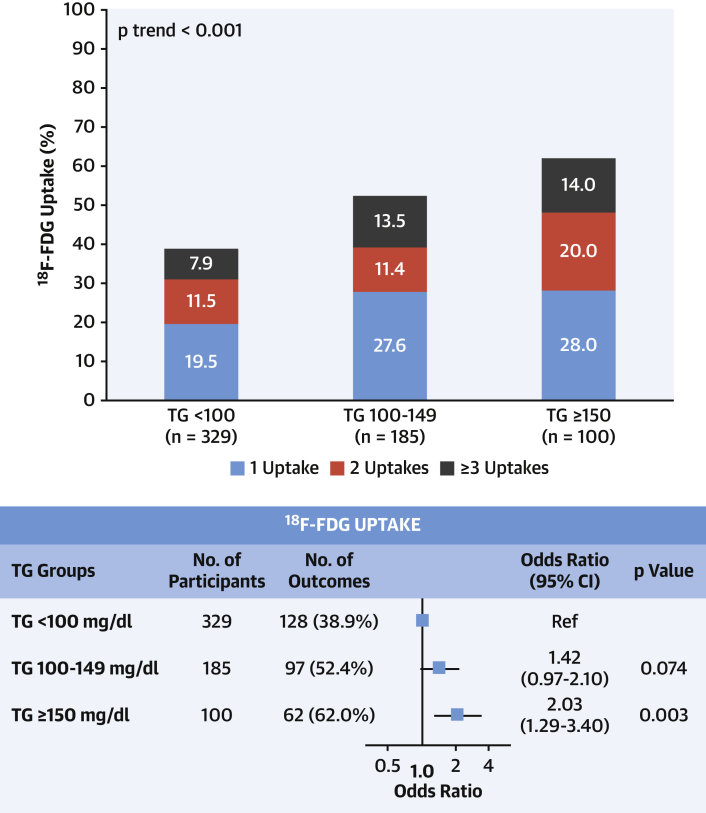
Results: Atherosclerotic plaques and CAC were observed in 58.0% and 16.8% of participants, respectively, whereas vascular inflammation was evident in 46.7% of evaluated participants. After multivariate adjustment, TG levels ≥150 mg/dl showed an association with subclinical noncoronary atherosclerosis (odds ratio [OR]: 1.35; 95% confidence interval [CI]: 1.08 to 1.68; p = 0.008). This association was significant for groups with high LDL-C (OR: 1.42; 95% CI: 1.11 to 1.80; p = 0.005) and normal LDL-C (OR: 1.85; 95% CI: 1.08 to 3.18; p = 0.008). No association was found between TG level and CAC score. TG levels ≥150 mg/dl were significantly associated with the presence of arterial inflammation (OR: 2.09; 95% CI: 1.29 to 3.40; p = 0.003).
Conclusions: In individuals with low to moderate cardiovascular risk, hypertriglyceridemia was associated with subclinical atherosclerosis and vascular inflammation, even in participants with normal LDL-C levels. (Progression of Early Subclinical Atherosclerosis [PESA]; NCT01410318).
Keywords: CACS; arterial inflammation; coronary calcification; subclinical atherosclerosis; triglycerides.
Copyright © 2021 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures The PESA study is funded by the National Center for Cardiovascular Research (CNIC) and Santander Bank. The study also has received funding from the Carlos III Health Institute (ISCIII; PI15/02019, PI17/00590, and PI20/00819) and the European Regional Development Fund. The CNIC is supported by the ISCIII, the Ministry of Science and Innovation, and the Pro CNIC Foundation. CNIC is a Severo Ochoa Center of Excellence (SEV-2015-0505). The funders had no role in the design and conduct of the study; the collection, management, analysis, and interpretation of the data; the preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication. Dr. Ibáñez is the recipient of a European Research Council grant MATRIX (ERC-COG-2018-ID: 819775). All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Triglycerides and Atherosclerosis: Bringing the Association Into Sharper Focus.J Am Coll Cardiol. 2021 Jun 22;77(24):3042-3045. doi: 10.1016/j.jacc.2021.04.058. J Am Coll Cardiol. 2021. PMID: 34140108 Free PMC article. No abstract available.
References
-
- Lee H., Park J.B., Hwang I.C. Association of four lipid components with mortality, myocardial infarction, and stroke in statin-naive young adults: a nationwide cohort study. Eur J Prev Cardiol. 2020;27:870–881. - PubMed
-
- Fernandez-Friera L., Fuster V., Lopez-Melgar B. Vascular inflammation in subclinical atherosclerosis detected by hybrid PET/MRI. J Am Coll Cardiol. 2019;73:1371–1382. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
