

Colonic dialysis can influence gut flora to protect renal function in patients with pre-dialysis chronic kidney disease
- PMID: 34140540
- PMCID: PMC8211730
- DOI: 10.1038/s41598-021-91722-1
Colonic dialysis can influence gut flora to protect renal function in patients with pre-dialysis chronic kidney disease
Abstract
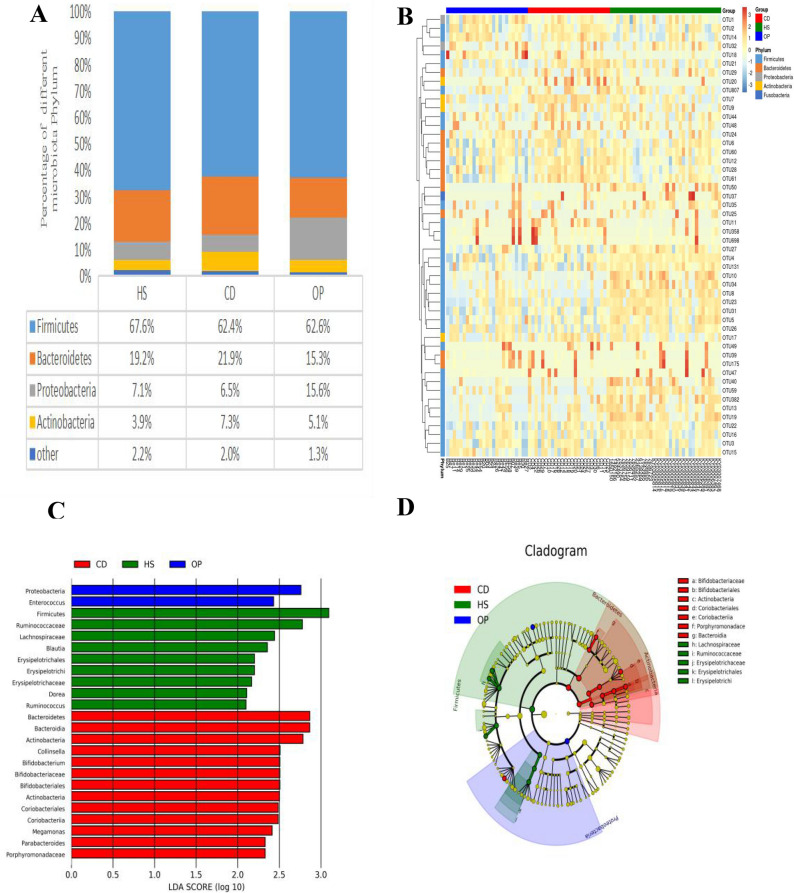
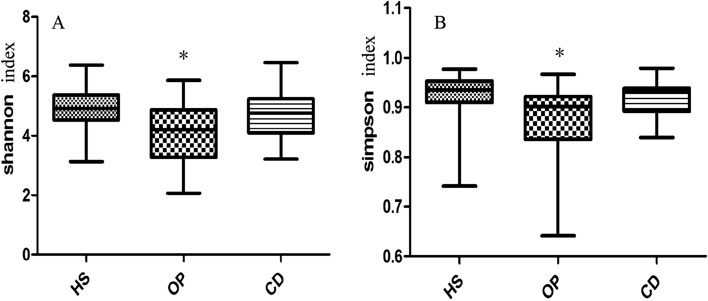
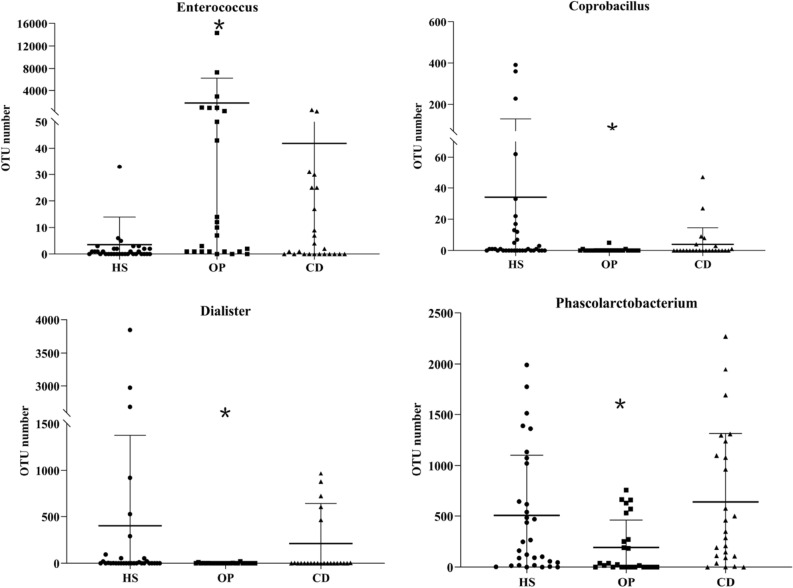
Chronic kidney disease (CKD) is a major public health burden around the world. The gut microbiome may contribute to CKD progression and serve as a promising therapeutic target. Colonic dialysis has long been used in China to help remove gut-derived toxins to delay CKD progression. Since disturbances in the gut biome may influence disease progression, we wondered whether colonic dialysis may mitigate the condition by influencing the biome. We compared the gut microbiota, based on 16S rRNA gene sequencing, in fecal samples of 25 patients with CKD (stages 3-5) who were receiving colonic dialysis(group CD), 25 outpatients with CKD not receiving colonic dialysis(group OP), and 34 healthy subjects(group HS). Richness of gut microbiota was similar between patients on colonic dialysis and healthy subjects, and richness in these two groups was significantly higher than that in patients not on colonic dialysis. Colonic dialysis also altered the profile of microbes in the gut of CKD patients, bringing it closer to the profile in healthy subjects. Colonic dialysis may protect renal function in pre-dialysis CKD by mitigating dysbiosis of gut microbiota.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Stevens PE, Levin A, Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members Evaluation and management of chronic kidney disease: synopsis of the kidney disease: Improving global outcomes 2012 clinical practice guideline. Ann. Intern. Med. 2013;158(11):825–830. doi: 10.7326/0003-4819-158-11-201306040-00007. - DOI - PubMed
-
- Kolff WJ. New ways of treating uraemia. Br. Med. J. 1947;2(4538):1041–1041.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
