

Time-outcome relationship in acute large-vessel occlusion exists across all ages: subanalysis of RESCUE-Japan Registry 2
- PMID: 34140563
- PMCID: PMC8211644
- DOI: 10.1038/s41598-021-92100-7
Time-outcome relationship in acute large-vessel occlusion exists across all ages: subanalysis of RESCUE-Japan Registry 2
Erratum in
-
Author Correction: Time-outcome relationship in acute large-vessel occlusion exists across all ages: subanalysis of RESCUE-Japan Registry 2.Sci Rep. 2021 Sep 8;11(1):18246. doi: 10.1038/s41598-021-97242-2. Sci Rep. 2021. PMID: 34497282 Free PMC article. No abstract available.
Abstract
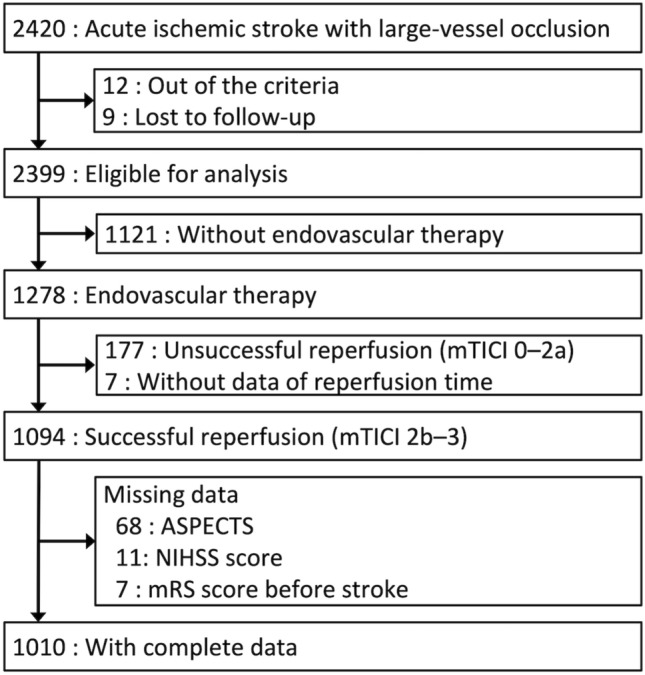
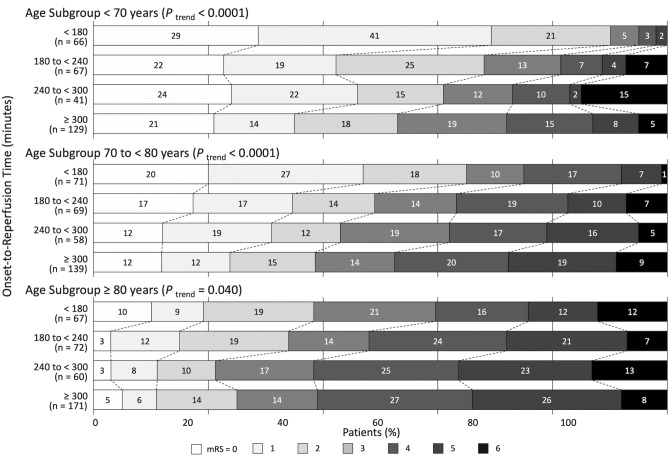
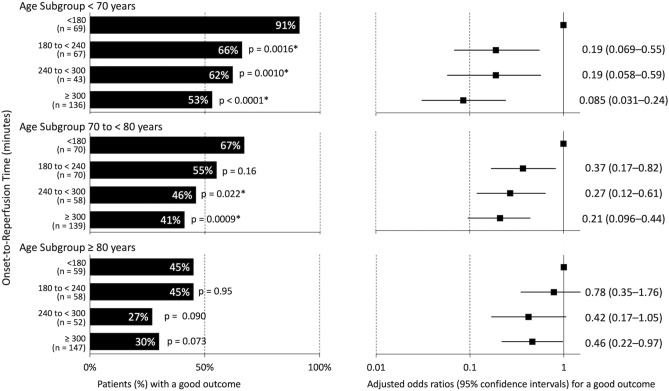
Early reperfusion after endovascular thrombectomy is associated with an improved outcome in ischemic stroke patients; however, the time dependency in elderly patients remains unclear. We investigated the time-outcome relationships in different age subgroups. Of 2420 patients enrolled in the RESCUE-Japan Registry 2 study, a study based on a prospective registry of stroke patients with acute cerebral large-vessel occlusion at 46 centers, we analyzed the data of 1010 patients with successful reperfusion after endovascular therapy (mTICI of 2b or 3). In 3 age subgroups (< 70, 70 to < 80, and ≥ 80 years), the mRS scores at 90 days were analyzed according to 4 categories of onset-to-reperfusion time (< 180, 180 to < 240, 240 to < 300, and ≥ 300 min). In each age subgroup, the distributions of mRS scores were better with shorter onset-to-reperfusion times. The adjusted common odds ratios for better outcomes per 1-category delay in onset-to-reperfusion time were 0.66 (95% CI 0.55-0.80) in ages < 70 years, 0.66 (95% CI 0.56-0.79) in ages 70 to < 80 years, and 0.83 (95% CI 0.70-0.98) in ages ≥ 80 years. Early reperfusion was associated with better outcomes across all age subgroups. Achieving early successful reperfusion is important even in elderly patients.
Conflict of interest statement
Dr. Todo reports lecturer fees from Medtronic and Stryker. Dr. Yoshimura reports research grants from Medico’s Hirata, Medtronic, and Termo and lecturer fees from Medtronic, Kaneka, and Stryker. Dr. Yamagami reports research grants from Bristol-Myers Squibb; lecturer fees from Stryker, Terumo, Medtronic, Medico’s Hirata, Johnson and Johnson, Bayer, Daiichi-Sankyo, Bristol-Myers Squibb, Boehringer Ingelheim, Takeda, and Otsuka Pharmaceutical; and membership in the advisory boards of Daiichi-Sankyo and Biomedical Solutions. Dr. Sakai reports a research grant from Termo, lecturer fees from Jimro, Johnson & Johnson, Medico’s Hirata, Medtronic, and Stryker; and membership in the advisory boards of Jimro and Medtronic. Dr. Nakamura reports lecturer fees from Johnson & Johnson, Medtronic, and Stryker. Dr. Kimura reports lecturer fees from Medtronic. Dr. Matsumaru discloses lecturer fees from Medtronic, Stryker, Terumo, Johnson & Johnson, Kaneka, and Jimro. Dr. Minematsu reports lecturer fees from Stryker and membership in the advisory board of Medico’s Hirata. The other authors report no conflicts related to the subject matter of the article.
Figures
References
-
- Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM, HERMES collaborators et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 2016;387:1723–1731. doi: 10.1016/S0140-6736(16)00163-X. - DOI - PubMed
-
- Muir KW, Ford GA, Messow CM, Ford I, Murray A, Clifton A, PISTE Investigators et al. Endovascular therapy for acute ischaemic stroke: the pragmatic ischaemic stroke thrombectomy evaluation (PISTE) randomised, controlled trial. J. Neurol. Neurosurg. Psychiatry. 2017;88:38–44. doi: 10.1136/jnnp-2016-314117. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
