

Incidence, electrophysiological characteristics, and long-term follow-up of perimitral atrial flutter in patients with previously confirmed mitral isthmus block
- PMID: 34141011
- PMCID: PMC8207388
- DOI: 10.1002/joa3.12545
Incidence, electrophysiological characteristics, and long-term follow-up of perimitral atrial flutter in patients with previously confirmed mitral isthmus block
Abstract
Introduction: After mitral isthmus (ΜΙ) catheter ablation, perimitral atrial flutter (PMF) circuits can be maintained due to the preservation of residual myocardial connections, even if conventional pacing criteria for complete MI block are apparently met (MI pseudo-block). We aimed to study the incidence, the electrophysiological characteristics, and the long-term outcome of these patients.
Methods: Seventy-two consecutive patients (mean age 62.4 ± 10.2, 62.5% male) underwent MI ablation, either as part of an atrial fibrillation (AF) ablation strategy (n = 35), or to treat clinical reentrant atrial tachycardia (AT) (n = 32), or to treat AT that occurred during ablation for AF (n = 5). Ιn all patients, the electrophysiological characteristics of PMF circuits were studied by high-density mapping.
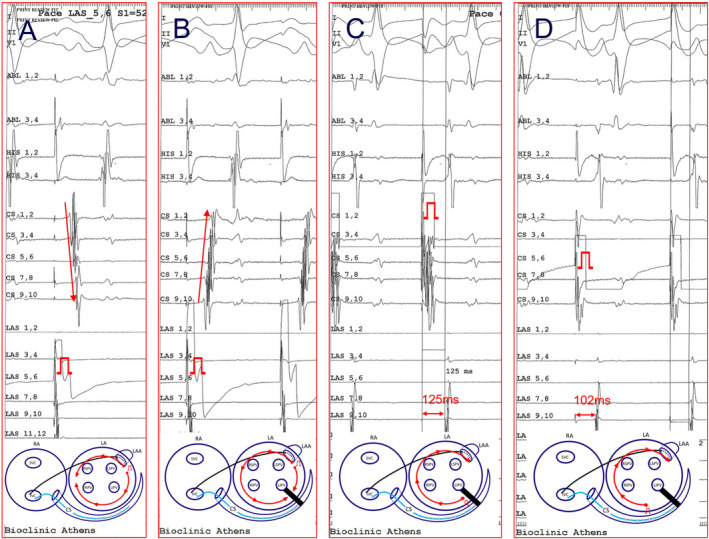
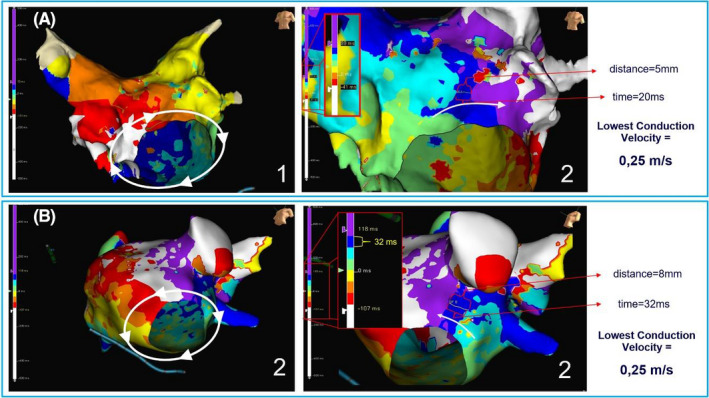
Results: Mitral isthmus block was successfully achieved in 69/72 patients (95.6%). Five patients developed PMF after confirming MI block. In these patients, high-density mapping during the PMF showed a breakthrough in MI with extremely low impulse conduction velocity (CV). In contrast, in usual PMF circuits that occurred after AF ablation, the lowest CV of the reentrant circuit was of significantly higher value (0.07 ± 0.02 m/s vs 0.25 ± 0.07 m/s, respectively; P < .001). Patients presented with clinical AT had better prognosis in maintaining sinus rhythm after MI ablation compared with patients presented with AF.
Conclusion: Perimitral atrial flutter with MI pseudo-block may be present after MI ablation and has specific electrophysiological features characterized by remarkably slow CV in the MI. Thus, even after MI block is achieved, a more detailed mapping in the boundaries of the ablation line or reinduction attempts may be needed to exclude residual conduction.
Keywords: atrial fibrillation; atrial tachycardias; catheter ablation; linear lesions; mitral isthmus; perimitral atrial flutter; pseudo‐block.
© 2021 The Authors. Journal of Arrhythmia published by John Wiley & Sons Australia, Ltd on behalf of Japanese Heart Rhythm Society.
Conflict of interest statement
The authors have no conflicts of interest relevant to this manuscript.
Figures




References
-
- Dukkipati S, Holmvang G, Ruskin J, Mansour M. Ablation of mitral isthmus‐dependent atrial flutter using integration of real‐time electroanatomic mapping with three‐dimensional computed tomography. Heart Rhythm. 2006;3(1):124. - PubMed
-
- Okamatsu H, Okumura K. Strategy and outcome of catheter ablation for persistent atrial fibrillation—impact of progress in the mapping and ablation technologies. Circ J. 2017;82(1):2–9. - PubMed
-
- Lo LW, Lin YJ, Chang SL, Hu YF, Chung FP, Chen SA. Beyond pulmonary vein isolation: the role of additional sites in catheter ablation of atrial fibrillation. Curr Cardiol Rep. 2017;19(9):86. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
