

Pediatric Acute Mastoiditis: Our Experience in a Tertiary Care Center
- PMID: 34141502
- PMCID: PMC8204207
- DOI: 10.7759/cureus.15052
Pediatric Acute Mastoiditis: Our Experience in a Tertiary Care Center
Abstract
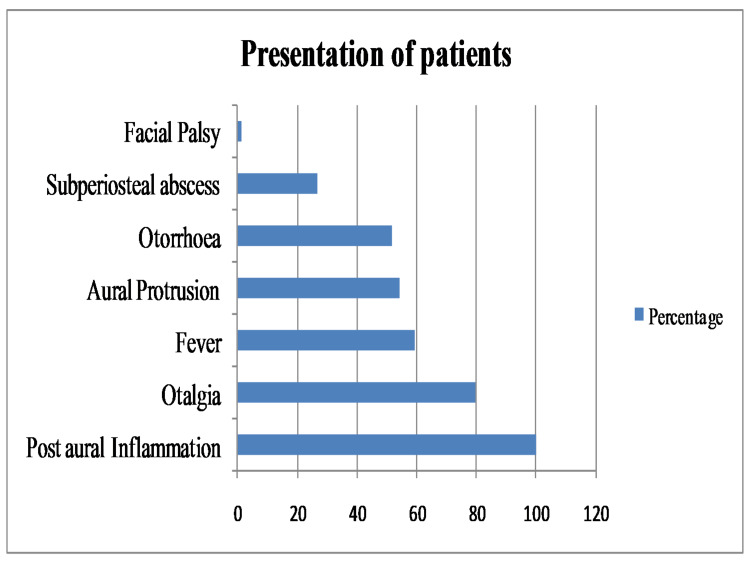
Introduction Acute mastoiditis (AM) is a common intra-temporal complication of acute otitis media (AOM) and is more commonly seen in children. Occasionally, it presents as the first sign of ear disease. This study aimed to evaluate the clinical course of AM and determine therapeutic options for pediatric patients presenting with AM. Methods This was a prospective, observational study conducted on patients with AM presenting at a tertiary center during one year period. Convenience sampling was employed and 79 pediatric patients (18 years or below) were recruited for the study. Data on the demographic profile of patients, the treatment offered, duration of hospital stay, and outcome were analyzed. Result In our study, 62% were male patients (n = 49) and 38% (n = 30) were females. The mean age of patients was 9.32 ± 5.3 years and a history of AOM was present in 60 (75.9%). On admission, the most common presentation was post-auricular inflammation (100%) followed by otalgia (79.7%), fever (59.5%), aural protrusion (54.4%), and otorrhoea (51.9%). Culture reports were available for 54 (68.4%) patients and 30 (38%) grew organisms. The cultured organisms were Streptococcus pneumonia (20.3%), Pseudomonas aeruginosa (10.1%), Streptococcus pyogenes (3.8%), and Staphylococcus aureus (3.8%). Most patients were managed conservatively (n = 66, 83.5%) whereas surgery was performed in 16.5% (n = 13) patients. The mean hospital stay was 5.58 ± 1.99 days. The need for surgical management was significantly associated with age >5 years (p = 0.006), history of AOM (p = 0.026) and the presence of complications (p = 0.012). Subperiosteal abscess (SA) was present in 21 (26.6%) patients and one had facial palsy. SA along with AM had a mean hospital stay of 8.5 ± 0.77 days compared to 4.94 ± 1.43 days in case of isolated AM (p < 0.001) and the mean age of presentation in SA with AM was 11.97 ± 5.13 years compared to 8.29 ± 5.14 years in case of isolated AM (p = 0.006). All patients recovered and were followed up to three months with no recurrence, complications, or sequelae. Conclusion Most of the cases of acute mastoiditis follow previous AOM episodes. With early recognition and effective treatment, the prognosis is good.
Keywords: acute mastoiditis; complications; management; nepal; pediatrics.
Copyright © 2021, Shrestha et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Similar articles
-
Acute mastoiditis in infancy: the Soroka experience: 1990-2000.Int J Pediatr Otorhinolaryngol. 2004 Nov;68(11):1435-9. doi: 10.1016/j.ijporl.2004.06.008. Int J Pediatr Otorhinolaryngol. 2004. PMID: 15488977
-
Our experience on the management of acute mastoiditis in pediatric acute otitis media patients.Int J Pediatr Otorhinolaryngol. 2020 Nov;138:110372. doi: 10.1016/j.ijporl.2020.110372. Epub 2020 Sep 7. Int J Pediatr Otorhinolaryngol. 2020. PMID: 32927353
-
Characteristics of CI children with complicated middle ear infections.Cochlear Implants Int. 2017 May;18(3):136-142. doi: 10.1080/14670100.2017.1289298. Epub 2017 Feb 24. Cochlear Implants Int. 2017. PMID: 28235386
-
Acute Mastoiditis Caused by Streptococcus pneumoniae.Pediatr Ann. 2016 May 1;45(5):e176-9. doi: 10.3928/00904481-20160328-01. Pediatr Ann. 2016. PMID: 27171806 Review.
-
Acute mastoiditis in children: review of the current status.Int J Pediatr Otorhinolaryngol. 2000 Nov 30;56(1):33-40. doi: 10.1016/s0165-5876(00)00406-7. Int J Pediatr Otorhinolaryngol. 2000. PMID: 11074113 Review.
Cited by
-
Pediatric Acute Mastoiditis: Which Factors Influence CT Scan Prescription and Surgical Intervention? A Multivariate Analysis.J Int Adv Otol. 2025 Jul 21;21(4):1-6. doi: 10.5152/iao.2025.251899. J Int Adv Otol. 2025. PMID: 40693582 Free PMC article.
-
A Child With Retroauricular Tenderness: Is It Really Mastoiditis?Cureus. 2023 May 23;15(5):e39394. doi: 10.7759/cureus.39394. eCollection 2023 May. Cureus. 2023. PMID: 37362478 Free PMC article.
References
-
- Acute mastoiditis in children as persisting problem. Djeric DR, Folic MM, Blazic SR, Djoric IB. J Int Adv Otol. 2014;10:60–63.
-
- Management of acute mastoiditis in children. A retrospective study and literature review. Abid W, Gamra OB, Ghorbal H, Cherif I, Zribi S, Hriga I, Mbarek C. Egypt J Ear Nose Throat Allied Sci. 2014;15:205–209.
-
- Algorithmic management of pediatric acute mastoiditis. Psarommatis IM, Voudouris C, Douros K, Giannakopoulos P, Bairamis T, Carabinos C. Int J Pediatr Otorhinolaryngol. 2012;76:791–796. - PubMed
-
- A contemporary analysis of acute mastoiditis. Gliklich RE, Eavey RD, Iannuzzi RA, Camacho AE. Arch Otolaryngol Head Neck Surg. 1996;122:135–139. - PubMed
-
- Acute mastoiditis in children: a seventeen-year experience in Dallas, Texas. Ghaffar FA, Wördemann M, McCracken GH Jr. Pediatr Infect Dis J. 2001;20:376–380. - PubMed
LinkOut - more resources
Full Text Sources