

Arthroscopic Bursa-Augmented Rotator Cuff Repair: A Vasculature-preserving Technique for Subacromial Bursal Harvest and Tendon Augmentation
- PMID: 34141532
- PMCID: PMC8185525
- DOI: 10.1016/j.eats.2021.01.013
Arthroscopic Bursa-Augmented Rotator Cuff Repair: A Vasculature-preserving Technique for Subacromial Bursal Harvest and Tendon Augmentation
Abstract
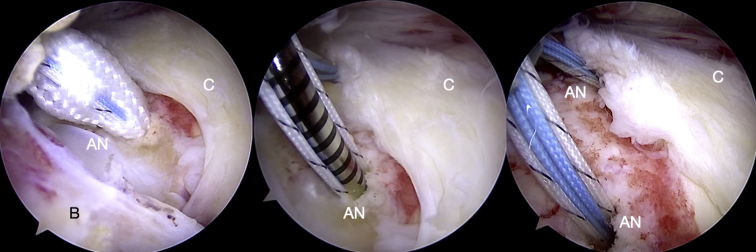
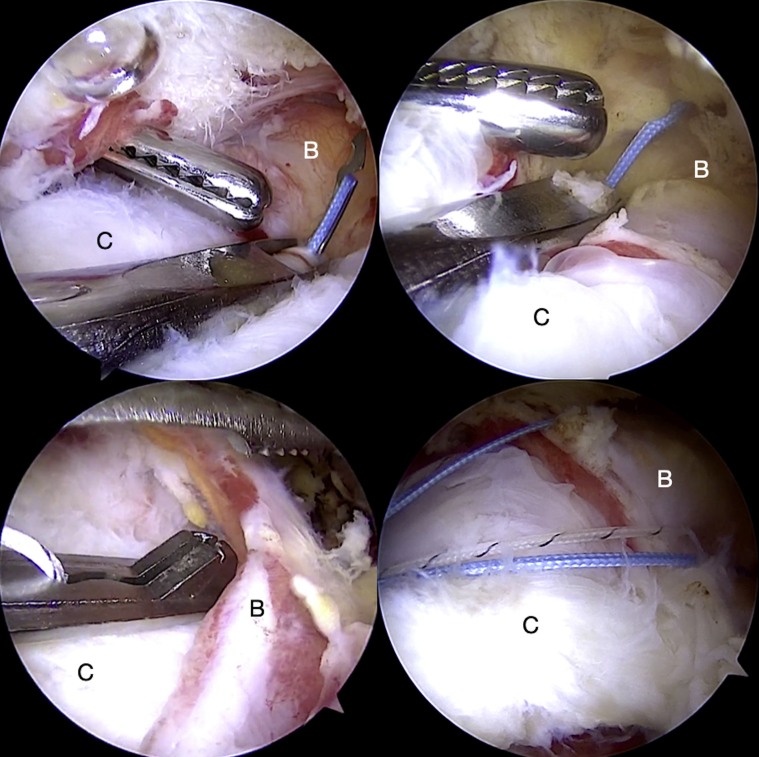
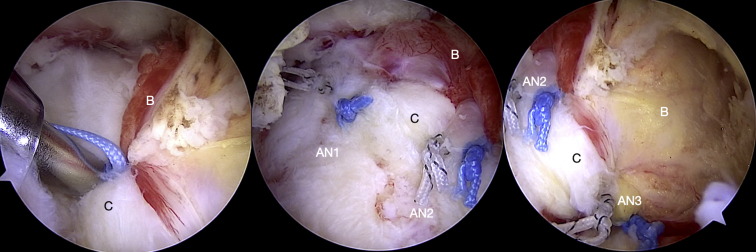
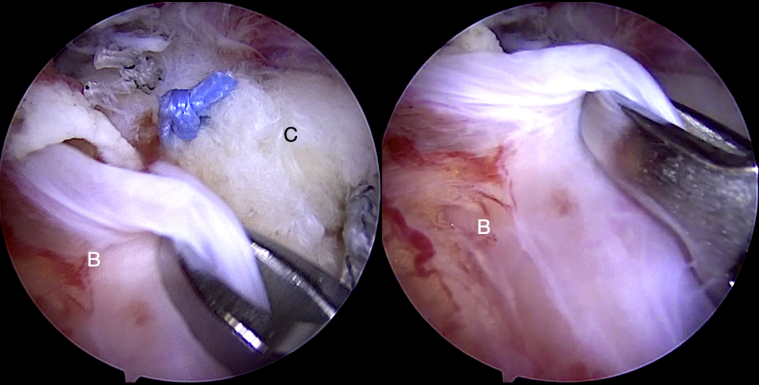
Rotator cuff repairs are associated with suboptimal outcomes and possibly greater incidence of retears if the biological healing environment is compromised. Strategies to optimize tendon-bone healing include the use of bioinductive scaffolds and regenerative stem cell therapy. The subacromial bursa has been shown to have significant pluripotent stem cell potency for tendon healing and has the advantage of easy accessibility and no added cost. However, a reproducible surgical technique for bursal mobilization, harvest, and vascularity preservation has not been described. We describe our technique for vasculature-preserving bursal mobilization and harvest of the entire posterosuperior and lateral subacromial bursa, and its use in rotator cuff repair augmentation is presented. The technique involves mobilization of the bursa as a continuous layer by maintain its medial and lateral vascularity. The bursa is advanced laterally, and the "vascular bursal duvet" and cuff tendons are repaired together as a tendon-bursa unit.
© 2021 by the Arthroscopy Association of North America. Published by Elsevier.
Figures
References
-
- Schlegel T.F., Abrams J.S., Bushnell B.D., Brock J.L., Ho C.P. Radiologic and clinical evaluation of a bioabsorbable collagen implant to treat partial-thickness tears: A prospective multicenter study. J Shoulder Elbow Surg. 2018;27:242–251. - PubMed
-
- Morikawa D., Muench L.N., Baldino J.B., et al. Comparison of preparation techniques for isolating subacromial bursa-derived cells as a potential augment for rotator cuff repair. Arthroscopy. 2020;36:80–85. - PubMed
-
- Chillemi C., Petrozza V., Franceschini V., et al. The role of tendon and subacromial bursa in rotator cuff tear pain: A clinical and histopathological study. Knee Surg Sports Traumatol Arthrosc. 2016;24:3779–3786. - PubMed
-
- Uhthoff H.K., Sarkar K. Surgical repair of rotator cuff ruptures. The importance of the subacromial bursa. J Bone Joint Surg Br. 1991;73:399–401. - PubMed
LinkOut - more resources
Full Text Sources
