

doi: 10.1016/j.eats.2021.01.020.
eCollection 2021 May.
Arthroscopic Excision of Bipartite Patella
Affiliations
- PMID: 34141540
- PMCID: PMC8185573
- DOI: 10.1016/j.eats.2021.01.020
Item in Clipboard
Arthroscopic Excision of Bipartite Patella
Arthrosc Tech.
.
Abstract
A bipartite patella usually presents as an incidental finding on radiographs because most cases are asymptomatic. However, some patients may present with pain and functional limitations. Conservative treatment is sufficient to resolve symptoms in most cases; however, a small minority of patients may require surgical management. Recent studies have reported excellent results with an arthroscopic approach. This Technical Note details our procedure for treating a symptomatic bipartite patella that has not resolved with conservative care.
© 2021 by the Arthroscopy Association of North America. Published by Elsevier.
Figures
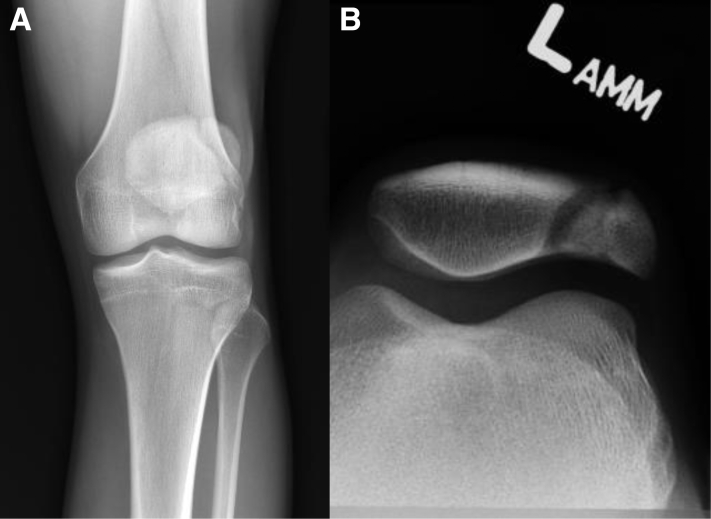
Anteroposterior (A) and sunrise (B) radiographs showing a bipartite patella in a right knee. The bipartite patella develops from an accessory ossification center in the patella—sometimes more than one. Typically, this developmental abnormality is asymptomatic and is discovered incidentally. However, in a minority of patients, pain over the superolateral, lateral, or inferior aspect of the patella and pain with activity may be caused by irritation. (A) Anteroposterior radiograph showing a patella with a superolateral fragment connected to the main body of the patella by a radiolucent band. (B) Sunrise view of same knee. The accessory patellar fragment can be seen extending far laterally, with a projection extending over the lateral femoral condyle. The arrows indicate the accessory portion of the bipartite patella. L, left.
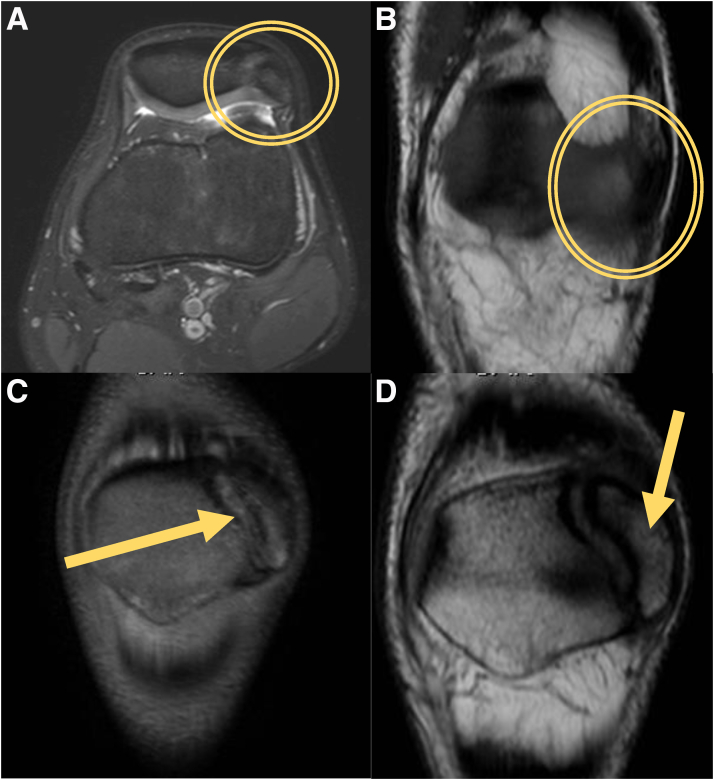
Magnetic resonance imaging (MRI) showing bipartite patella. (A) Axial MRI of the left knee shows an accessory patellar fragment (circle). (B) Coronal MRI of the same knee shows a deeper lateral portion of the accessory part of the bipartite patella (circle). (C) A more superficial cut on coronal MRI of the same knee shows a large superolateral patellar fragment (arrow). (D) T1 coronal MRI of the left knee with clearly delineated outline of the patellar fragment with malunion (arrow). The bipartite patella is a developmental abnormality that is often asymptomatic. Most cases of symptomatic bipartite patella are amenable to conservative management, but in a minority of these patients, surgical intervention is needed.

Diagnostic arthroscopy: view of bipartite patella. This arthroscopic view is through the anteromedial portal, looking at the lateral undersurface of the patella. Visible are the main body of the patella, the unfused accessory portion, and the lateral retinacular structures. The fibrocartilaginous seam (arrow) between the main body of the patella and the non-unionized fragment(s) will be the line of excision.

Bipartite patella fragment excision. Excision of a non-unionized patellar fragment is undertaken when the patient is symptomatic and resistant to conservative management with activity modification, physical therapy, and nonsteroidal anti-inflammatory drugs. In this patient, the working portal is the lateral portal; most cases of bipartite patella involve a superolateral fragment. These views are from the medial portal of the lateral undersurface of the patella. (A) A spinal needle is pushed through the fibrocartilaginous seam between the main body of the patella and the non-unionized fragment; this may make the resection easier. (B) A small high-speed burr is used to resect along the same line. (C) An elevator is used to remove part of the fragment. These implements, along with arthroscopic shavers and larger arthroscopic burrs, are used to either disintegrate the non-unionized fragment or cut along its connection with the main body of the patella. Pieces of the fragment are removed with arthroscopic graspers as able.

Exterior pressure on patella. Arthroscopic excision of non-unionized patellar fragments in patients with a symptomatic bipartite patella is sometimes difficult because of the thickness and durability of the tissue between the body of the patella and the malunion fragment. An arthroscopic approach is preferred to decrease the recovery time and minimize scarring and morbidity for the patient, but the limitations of an arthroscopic approach mean that this procedure can lead to a lengthy tourniquet time. Pressure from the exterior against the patella can be applied with the surgeon’s thumb (arrow)—or with the aid of an assistant—to maximize the force of the burr and gain more purchase to resect the fragment.

Intraoperative and postoperative imaging after arthroscopic bipartite patella excision. A symptomatic bipartite patella is rare and usually can be treated nonoperatively. In a small minority of patients, surgical excision is necessary; this is often performed arthroscopically. (A) Intraoperative fluoroscopy of a left knee verifies adequate resection of accessory patellar fragments (arrow). (B) Postoperative anteroposterior radiography of the same knee shows a resected bipartite patella (arrow).
References
-
- McMahon S.E., LeRoux J.A., Smith T.O., Hing C.B. The management of the painful bipartite patella: A systematic review. Knee Surg Sports Traumatol Arthrosc. 2016;24:2798–2805. - PubMed
-
- Oohashi Y. Developmental anomaly of ossification type patella partita. Knee Surg Sports Traumatol Arthrosc. 2015;23:1071–1076. - PubMed
-
- Kavanagh E.C., Zoga A., Omar I., Ford S., Schweitzer M., Eustace S. MRI findings in bipartite patella. Skeletal Radiol. 2007;36:209–214. - PubMed
-
- Oohashi Y., Koshino T., Oohashi Y. Clinical features and classification of bipartite or tripartite patella. Knee Surg Sports Traumatol Arthrosc. 2010;18:1465–1469. - PubMed
-
- James E.W., LaPrade C.M., Chahla J., Cinque M.E., Kennedy N.I., LaPrade R.F. Arthroscopic excision of bipartite patella with preservation of lateral retinaculum in an adolescent ice hockey player. Am J Orthop. 2017;46:135–138. - PubMed
LinkOut - more resources
Full Text Sources
