

Implementation of an Infectious Diseases Telehealth Consultation and Antibiotic Stewardship Program for 16 Small Community Hospitals
- PMID: 34141816
- PMCID: PMC8205263
- DOI: 10.1093/ofid/ofab168
Implementation of an Infectious Diseases Telehealth Consultation and Antibiotic Stewardship Program for 16 Small Community Hospitals
Abstract
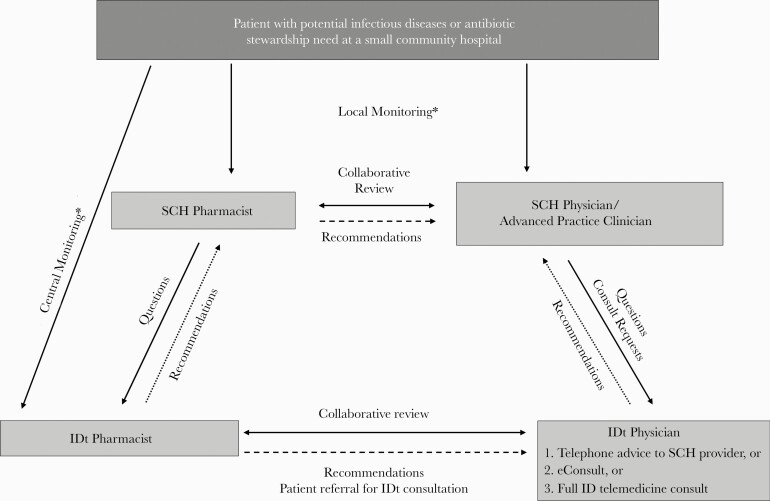
Background: Telehealth improves access to infectious diseases (ID) and antibiotic stewardship (AS) services in small community hospitals (SCHs), but the optimal model has not been defined. We describe implementation and impact of an integrated ID telehealth (IDt) service for 16 SCHs in the Intermountain Healthcare system.
Methods: The Intermountain IDt service included a 24-hour advice line, eConsults, telemedicine consultations (TCs), daily AS surveillance, long-term AS program (ASP) support by an IDt pharmacist, and a monthly telementoring webinar. We evaluated program measures from November 2016 through April 2018.
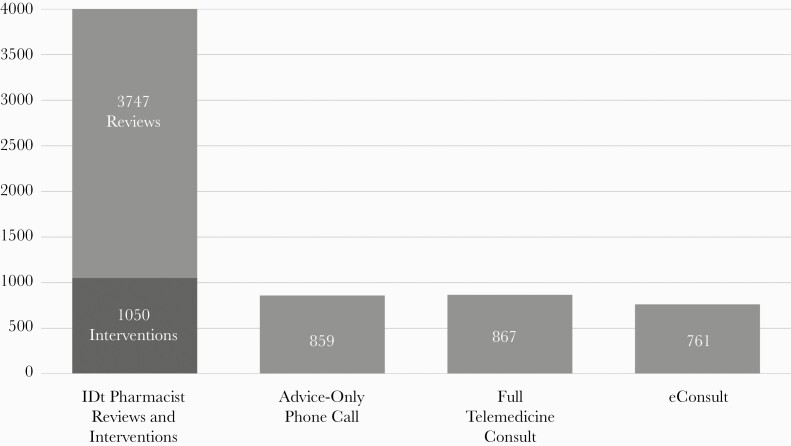
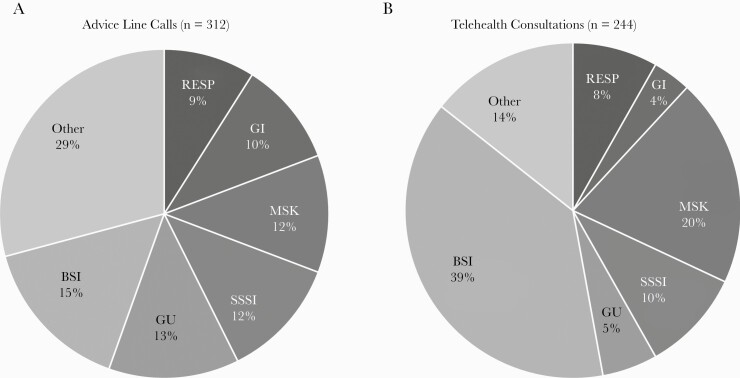
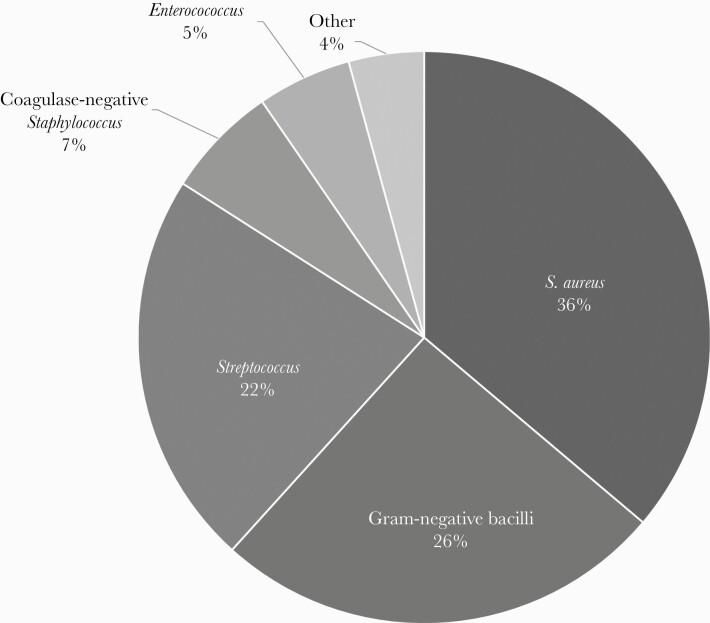
Results: A total of 2487 IDt physician interactions with SCHs were recorded: 859 phone calls (35% of interactions), 761 eConsults (30%), and 867 TCs (35%). Of 1628 eConsults and TCs, 1400 (86%) were SCH provider requests, while 228 (14%) were IDt pharmacist generated. Six SCHs accounted for >95% of interactions. Median consultation times for each initial telehealth interaction type were 5 (interquartile range [IQR], 5-10) minutes for phone calls, 20 (IQR, 15-25) minutes for eConsults, and 50 (IQR, 35-60) minutes for TCs. Thirty-two percent of consults led to in-person ID clinic follow-up. Bacteremia was the most common reason for consultation (764/2487 [31%]) and Staphylococcus aureus the most common organism identified. ASPs were established at 16 facilities. Daily AS surveillance led to 2229 SCH pharmacist and 1305 IDt pharmacist recommendations. Eight projects were completed with IDt pharmacist support, leading to significant reductions in meropenem, vancomycin, and fluoroquinolone use.
Conclusions: An integrated IDt model led to collaborative ID/ASP interventions and improvements in antibiotic use at 16 SCHs. These findings provide insight into clinical and logistical considerations for IDt program implementation.
Keywords: antibiotic stewardship; community hospital; critical access hospitals; infectious diseases; telehealth.
© The Author(s) 2021. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures
References
-
- Schmitt S, McQuillen DP, Nahass R, et al. . Infectious diseases specialty intervention is associated with decreased mortality and lower healthcare costs. Clin Infect Dis 2014; 58:22–8. - PubMed
-
- Stenehjem E, Hyun DY, Septimus E, et al. . Antibiotic stewardship in small hospitals: barriers and potential solutions. Clin Infect Dis 2017; 65:691–6. - PubMed
-
- Young JD, Abdel-Massih R, Herchline T, et al. . Infectious Diseases Society of America position statement on telehealth and telemedicine as applied to the practice of infectious diseases. Clin Infect Dis 2019; 68:1437–43. - PubMed
-
- Centers for Disease Control and Prevention. Core elements of hospital antibiotic stewardship programs. Available at: https://www.cdc.gov/antibiotic-use/core-elements/hospital.html. Accessed 20 April 2020. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
