

Dots, lines, contours, and ends: An image-based review of esophageal pathology
- PMID: 34141830
- PMCID: PMC8187835
- DOI: 10.1016/j.ejro.2021.100361
Dots, lines, contours, and ends: An image-based review of esophageal pathology
Abstract
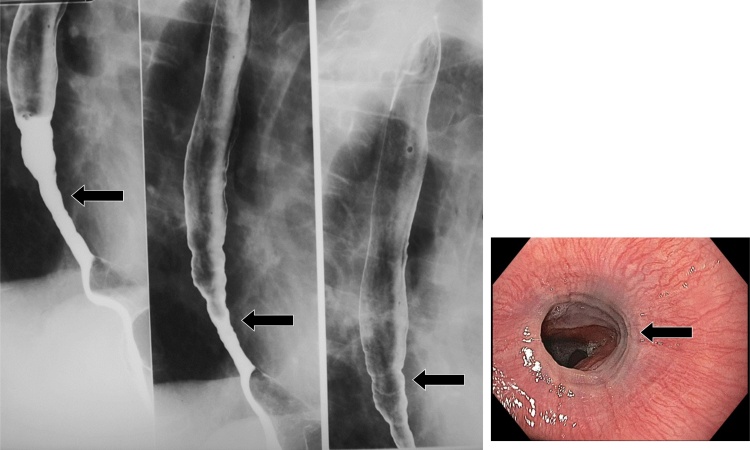
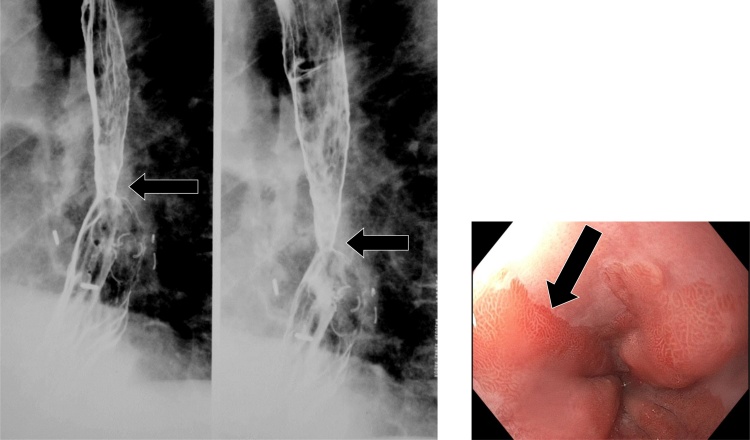
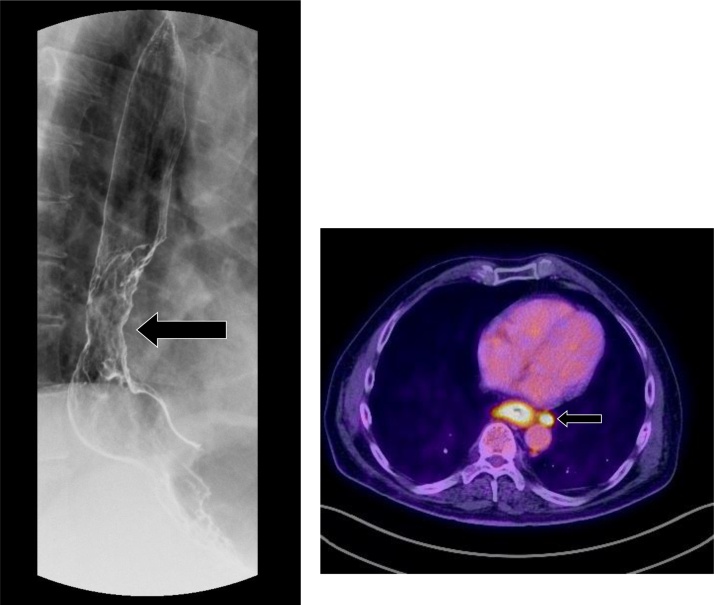
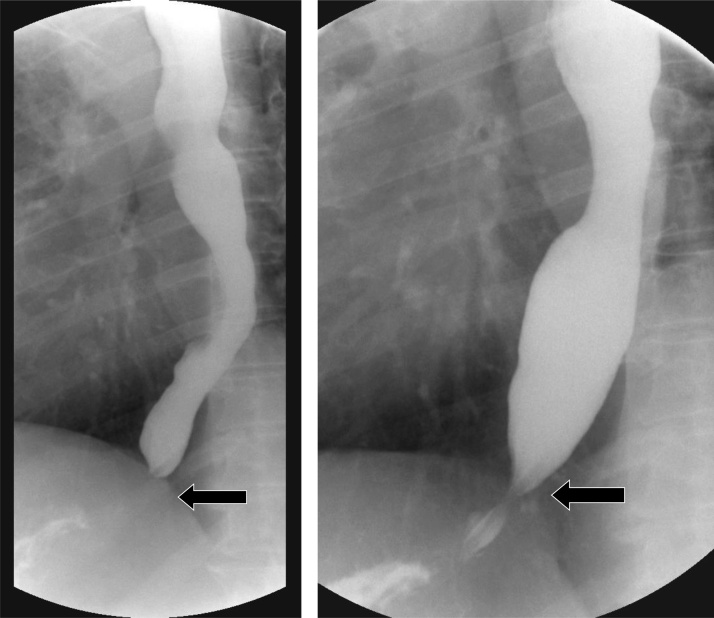
Esophageal pathologies encountered on fluoroscopic examination may pose a diagnostic challenge to the interpreting Radiologist. Understanding the varied imaging appearances of esophageal pathology requires a thorough understanding of barium esophagography. This article reviews the various fluoroscopic imaging findings of different esophageal pathologies by describing an approach to image interpretation centered on dots, lines, contours, and ends. By utilizing this approach, the Radiologist will be better positioned to reconcile seemingly disparate pathologies into a cogent and succinct differential diagnosis.
Keywords: Fluoroscopy; Oesophageal patterns; Oesophaghus; Oesophagram.
© 2021 The Authors.
Conflict of interest statement
There are no known conflicts of interest associated with this publication and there has been no financial support for this work. All authors explicitly approve the content within this manuscript.
Figures



















References
-
- Levine M.S., Rubesin S.E. Diseases of the esophagus: diagnosis with esophagography. Radiology. 2005;237(November (2)):414–427. Radiology. 2005 Nov;237(2):414-427. - PubMed
-
- Gore R.M., Levine M.S. 4th edition. Saunders; 2014. Textbook of Gastrointestinal Radiology. December 10.
-
- Levine M.S., Ramchandani P., Rubesin S.E. Cambridge University Press; 2012. Practical Fluoroscopy of the GI and GU Tracts.
-
- Noh H.M., Fishman E.K., Forastiere A.A., Bliss D.F., Calhoun P.S. CT of the esophagus: spectrum of disease with emphasis on esophageal carcinoma. Radiographics. 1995;15(September (5)):1113–1134. - PubMed
-
- Hoversten P., Kamboj A.K., Katzka D.A. Infections of the esophagus: an update on risk factors, diagnosis, and management. Dis. Esophagus. 2018;31(December (12)) - PubMed
Publication types
LinkOut - more resources
Full Text Sources
