

Chronically elevated branched chain amino acid levels are pro-arrhythmic
- PMID: 34142125
- PMCID: PMC9215196
- DOI: 10.1093/cvr/cvab207
Chronically elevated branched chain amino acid levels are pro-arrhythmic
Abstract
Aims: Cardiac arrhythmias comprise a major health and economic burden and are associated with significant morbidity and mortality, including cardiac failure, stroke, and sudden cardiac death (SCD). Development of efficient preventive and therapeutic strategies is hampered by incomplete knowledge of disease mechanisms and pathways. Our aim is to identify novel mechanisms underlying cardiac arrhythmia and SCD using an unbiased approach.
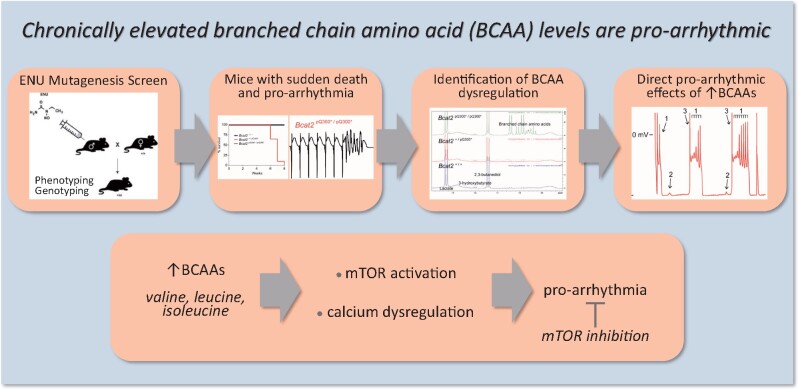
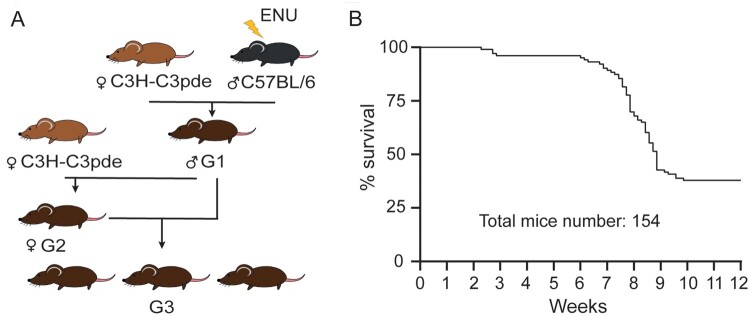
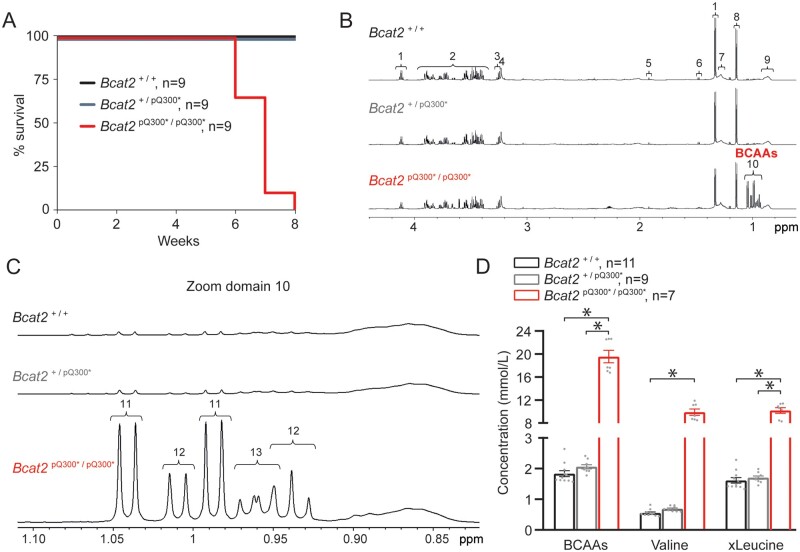
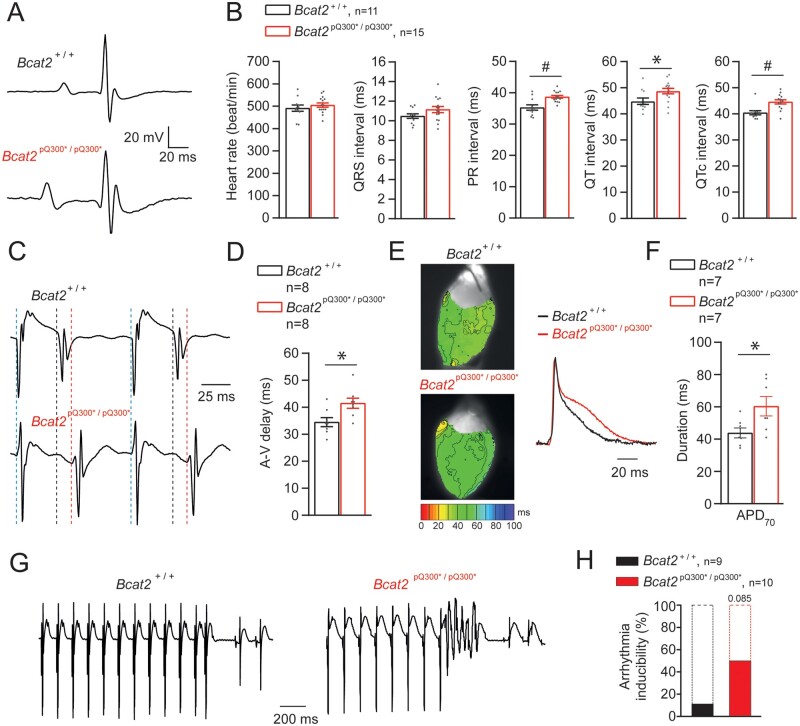
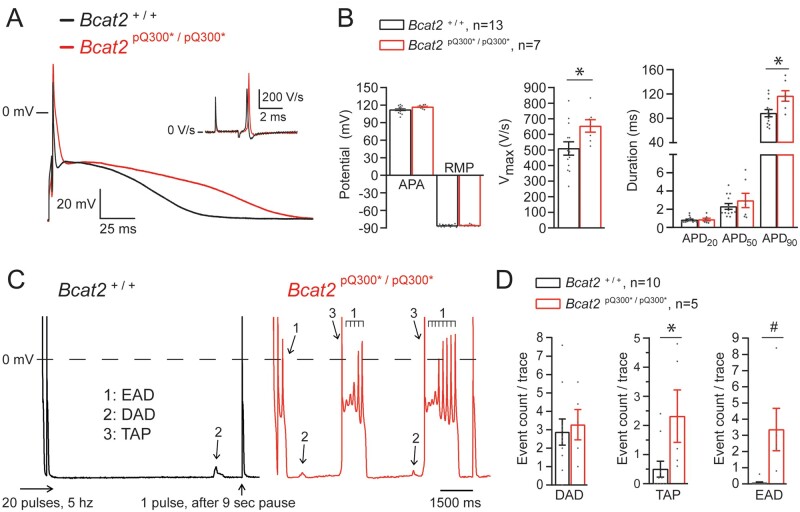
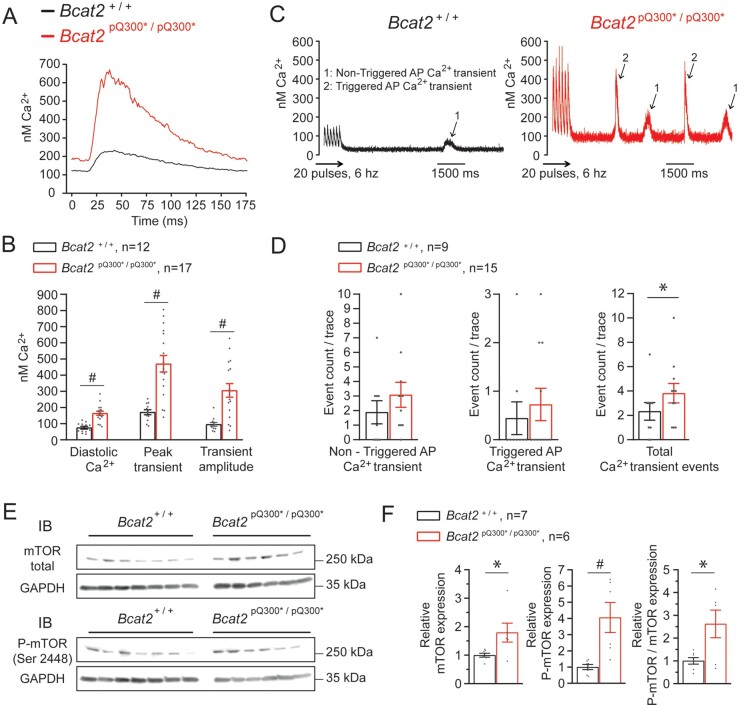
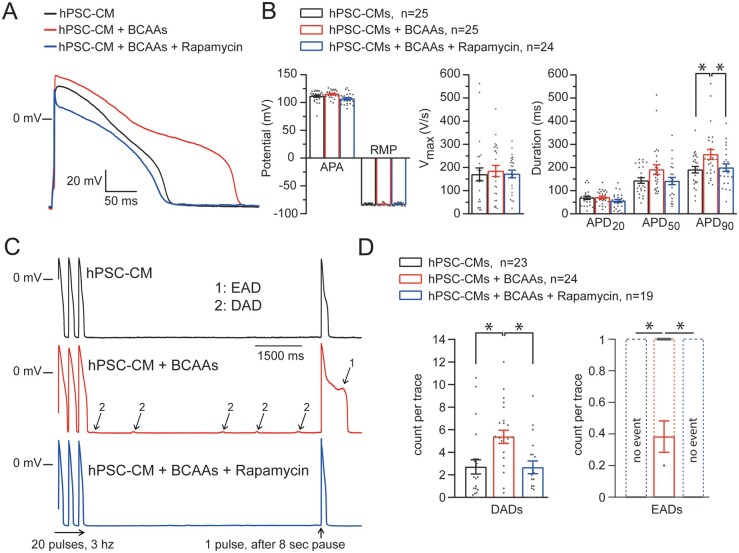
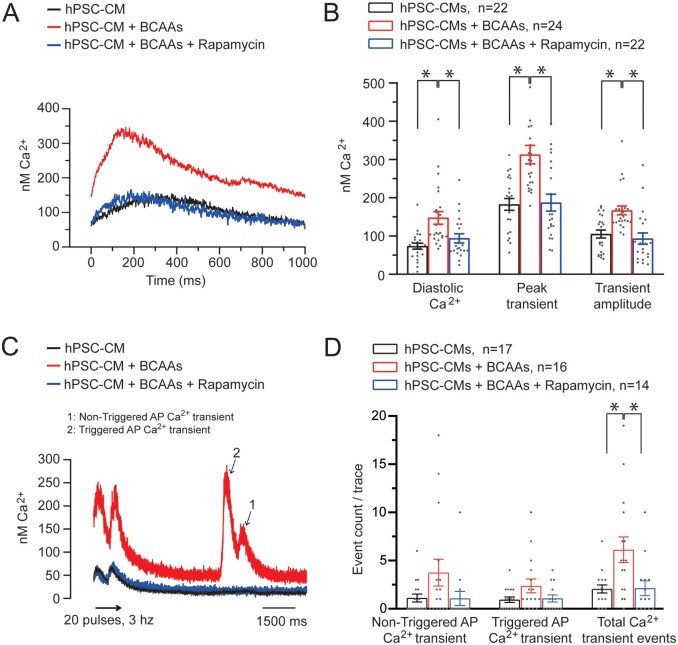
Methods and results: We employed a phenotype-driven N-ethyl-N-nitrosourea mutagenesis screen and identified a mouse line with a high incidence of sudden death at young age (6-9 weeks) in the absence of prior symptoms. Affected mice were found to be homozygous for the nonsense mutation Bcat2p.Q300*/p.Q300* in the Bcat2 gene encoding branched chain amino acid transaminase 2. At the age of 4-5 weeks, Bcat2p.Q300*/p.Q300* mice displayed drastic increase of plasma levels of branch chain amino acids (BCAAs-leucine, isoleucine, valine) due to the incomplete catabolism of BCAAs, in addition to inducible arrhythmias ex vivo as well as cardiac conduction and repolarization disturbances. In line with these findings, plasma BCAA levels were positively correlated to electrocardiogram indices of conduction and repolarization in the German community-based KORA F4 Study. Isolated cardiomyocytes from Bcat2p.Q300*/p.Q300* mice revealed action potential (AP) prolongation, pro-arrhythmic events (early and late afterdepolarizations, triggered APs), and dysregulated calcium homeostasis. Incubation of human pluripotent stem cell-derived cardiomyocytes with elevated concentration of BCAAs induced similar calcium dysregulation and pro-arrhythmic events which were prevented by rapamycin, demonstrating the crucial involvement of mTOR pathway activation.
Conclusions: Our findings identify for the first time a causative link between elevated BCAAs and arrhythmia, which has implications for arrhythmogenesis in conditions associated with BCAA metabolism dysregulation such as diabetes, metabolic syndrome, and heart failure.
Keywords: Arrhythmia; BCAA; Electrophysiology; Metabolism; Sudden death.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Priori SG, Blomström-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, Elliott PM, Fitzsimons D, Hatala R, Hindricks G, Kirchhof P, Kjeldsen K, Kuck K-H, Hernandez-Madrid A, Nikolaou N, Norekvål TM, Spaulding C, Veldhuisen DV; ESC Scientific Document Group .2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: the Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J 2015;36:2793–2867. - PubMed
-
- Hoeijen DV, Blom MT, Bardai A, Souverein PC, Boer AD, Tan HL.. Reduced pre-hospital and in-hospital survival rates after out-of-hospital cardiac arrest of patients with type-2 diabetes mellitus: an observational prospective community-based study. Europace 2015;17:753–760. - PubMed
-
- Jouven X, Lemaître RN, Rea TD, Sotoodehnia N, Empana J-P, Siscovick DS.. Diabetes, glucose level, and risk of sudden cardiac death. Eur Heart J 2005;26:2142–2147. - PubMed
-
- Tomaselli GF, Zipes DP.. What causes sudden death in heart failure? Circ Res 2004;95:754–763. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
