

Diagnostic interval for non-screening patients undergoing mammography during the COVID-19 pandemic
- PMID: 34143286
- PMCID: PMC8211559
- DOI: 10.1007/s00330-021-08117-z
Diagnostic interval for non-screening patients undergoing mammography during the COVID-19 pandemic
Abstract
Objective: During the COVID-19 pandemic, there was a temporary cessation of mammography screening. However, in some facilities, diagnostic breast imaging services continued for patients with a high clinical suspicion of breast cancer. The objective of this study was to evaluate changes in the diagnostic interval (DI) of non-screening patients presenting for diagnostic mammography during the first wave of the COVID-19 pandemic.
Methods: Retrospective chart review was performed on patients presenting for non-screening diagnostic mammography from April 1 to June 30, 2020 (pandemic group) and April 1 to June 30, 2019 (pre-pandemic group). Age, reason for referral, number and type of imaging studies/biopsies necessary for a final diagnosis were recorded. Diagnostic interval (DI) was defined as the number of days from the date of the diagnostic mammogram to the date of the final diagnosis.
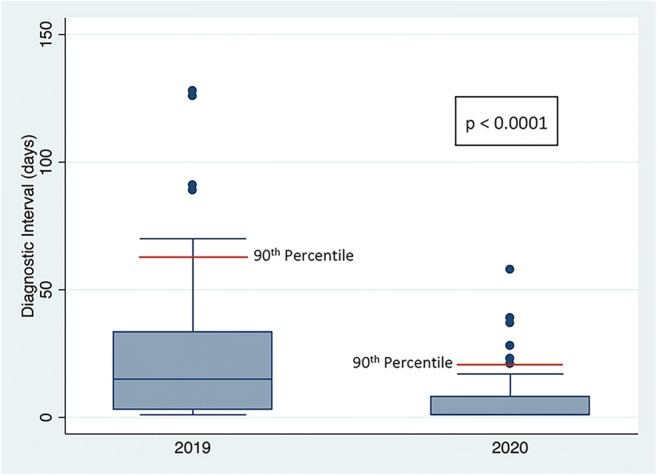
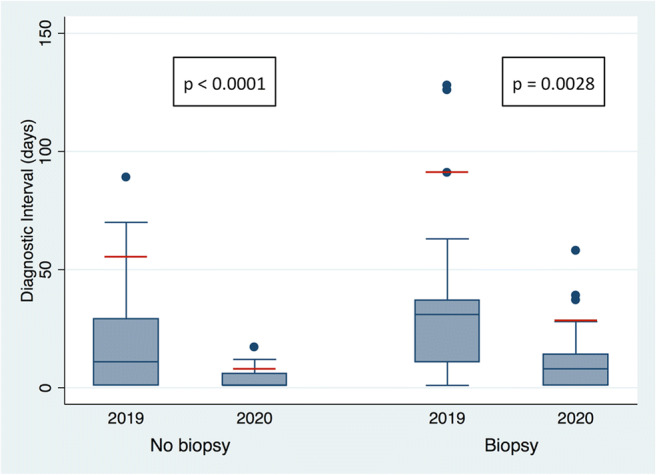
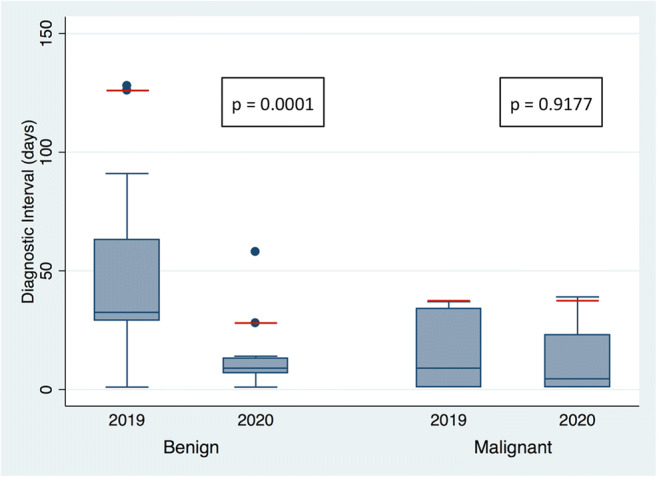
Results: Compared to the pre-pandemic group (n = 64), the pandemic group (n = 77) showed a reduction in DI of the entire cohort (pandemic: 1 day; pre-pandemic: 15 days, p < 0.0001) for patients not requiring tissue sampling (pandemic: 1 day; pre-pandemic: 11 days, .p < 0.0001) and those requiring tissue sampling with benign pathology (pandemic 9 days; pre-pandemic, 33 days, p = 0.0002). A higher percentage of patients in the pandemic group had their assessment completed during the initial visit (pandemic: 50.6%; pre-pandemic: 23.4%, p = 0.0009).
Conclusion: During the first wave of the COVID-19 pandemic, the DI for patients with non-screening-related diagnostic mammography was significantly shorter, with a higher percentage of patients completing their assessments on the initial visit, compared to one year prior.
Key points: • Despite reductions in manpower and clinical services, during pandemic times, it is possible to maintain a diagnostic breast imaging service for women at high clinical suspicion for breast cancer. • During pandemic times, breast imaging departments should consider restructuring to a Rapid Diagnostic Unit model with a navigation team that follows patients through the assessment process to a final diagnosis. • Departmental restructuring and patient navigation during pandemic times could either maintain or shorten the diagnostic interval for patients presenting for diagnostic mammography.
Keywords: Breast; COVID-19; Diagnostic interval; Mammogram.
© 2021. European Society of Radiology.
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures
References
-
- Feletto E, Grogan P, Nickson C et al (2020) How has COVID-19 impacted cancer screening? Adaptation of services and the future outlook in Australia. Public Health Res Pract 30(4):3042026. 10.17061/phrp3042026 - PubMed
-
- McKibbin, Warwick J. and Fernando, Roshen, The Global Macroeconomic Impacts of COVID-19: Seven Scenarios (March 2, 2020). CAMA Working Paper No. 19/2020, Available at 10.2139/ssrn.3547729
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
